
Rationale and Objectives
Both magnetic resonance (MR) and computed tomographic (CT) colonography are useful for colon examination. With sensitivities close to those for conventional colonoscopy (CC) for polyps, colonography has been proposed as an alternative to diagnostic CC. MR colonography (MRC) with fecal tagging may be a method of gaining further patient acceptance and widespread use, but the method has to be optimized. The aim of our study was to evaluate the quality of a new contrast agent mixture and to validate a new method for evaluating the tagging efficiency of contrast agents.
Materials and Methods
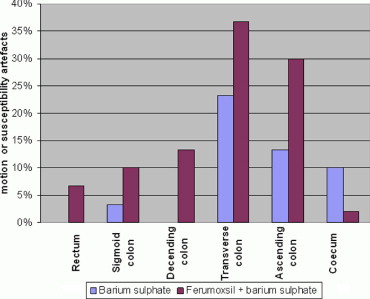
Twenty patients referred to CC underwent dark lumen MRC prior to the colonoscopy. Two groups of patients received two different oral contrast agents (barium sulfate and barium sulfate/ferumoxsil) as a laxative-free fecal tagging prior to the MRC. After MRC, the contrast agent was rated qualitatively (with the standard method using contrast-to-wall ratio) and subjectively (using a visual analog scale [VAS]) by three different blinded observers.
Results
Evaluated both qualitatively and subjectively, the tagging efficiency of barium sulfate/ferumoxsil was significantly better ( P < .05) than barium sulfate alone. The VAS method for evaluating the tagging efficiency of contrast agents showed a high correlation (observer II, r = 0.91) to the standard method using contrast-to-wall ratio and also a high interclass correlation (observer II and III = 0.89/0.85). MRC found 1 of 22 (5%) polyps <6 mm, 2 of 3 (67%) polyps 6−10 mm, and 2 of 2 (100%) polyps >10 mm.
Conclusion
MRC with fecal tagging using barium sulfate/ferumoxsil as contrast agent will give better overall assessment of the colon wall compared to barium sulfate alone. Furthermore, the VAS method of evaluating fecal tagging efficiency correlated with the standard method of calculating the contrast-to-wall ratio.
Ever since the development of magnetic resonance (MR) and computed tomographic (CT) colonography, the techniques have been labeled as promising new methods for examining the colon. It has been argued that with the high sensitivities of both CT and MR colonography, the techniques now stand as realistic alternatives or supplements to conventional colonoscopy (CC), which so far has remained the gold standard for colon examination. Considering the drawbacks of colonoscopies (colonic cleansing, pain, need for sedation, complication rates, mortality, etc.) and especially considering that studies have shown a potential decrease in mortality from colorectal cancer between 15% and 33% with screening of an asymptomatic population ( ), many have followed the development of MR and CT colonography with high expectations.
So far, several studies have been published describing MR colonography (MRC) with fecal tagging ( ), and some have suggested that that colonography with little or no colonic cleansing would improve patient acceptance, the rationale being that colonic cleansing for a majority of patients subjected to colonic examination is rated as one of the most uncomfortable parts of the procedure ( ).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Study Group
Get Radiology Tree app to read full this article<
Patient Preparation
Get Radiology Tree app to read full this article<
MR Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Contrast=(Istool−Iwall)/(Istool+Iwall), Contrast
=
(I
stool
−
I
wall
)
/
(
I
stool
+
I
wall
)
,
where I stool and I wall are correspondingly mean intensities of region of interest (ROI) placed in the stool and in the wall, respectively. Signal intensity was measured using a circular ROI of 100 mm 2 in the stool and using free-hand ROI of 50 mm 2 in the colonic wall. The circular ROI was placed by the evaluators in the stool that was judged to be representative for the whole segment. The free-hand ROI was placed in the proximity of the circular ROI. For polyps and tumors and location/size of lesions, the six segments of the colon were evaluated by consensus decision by V.B.L. and M.P.A.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conventional Colonoscopy
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Subjective Evaluation of Tagging Efficiency and Diagnostic Confidence for All Observers
Tagging Efficiency VAS Diagnostic Confidence VAS Rectum Sigmoid Colon Descending Colon Transverse Colon Ascending Colon Cecum Rectum Sigmoid Colon Descending Colon Transverse Colon Ascending Colon Cecum Group A ⁎ 4.4 4.3 4.3 4.0 4.3 4.5 7.2 6.8 7.0 6.7 6.7 5.9 Group B † 8.0 8.0 8.0 7.7 7.2 7.1 8.2 8.6 8.6 7.9 7.5 6.9P -value ‡ <.001 <.0001 <.0001 <.0001 <.0001 <.001 <.003 <.0001 <.0001 <.006 <.27 <.076
Tagging efficiency and diagnostic confidence was evaluated using VAS, a continuous scale from 0 to 10 (0 = no tagging, 10 = optimal tagging).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Qualitative Evaluation of Tagging Efficiency for All Observers
Tagging Efficiency VAS Rectum Sigmoid Colon Descending Colon Transverse Colon Ascending Colon Cecum Group A ⁎ 0.19 0.17 0.18 0.23 0.21 0.29 Group B † 0.42 0.64 0.43 0.54 0.45 0.42P -value ‡ <.002 <.0001 <.0001 <.0001 <.0002 .05
Tagging efficiency and diagnostic confidence was evaluated using VAS, a continuous scale from 0 to 10 (0 = no tagging, 10 = optimal tagging).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
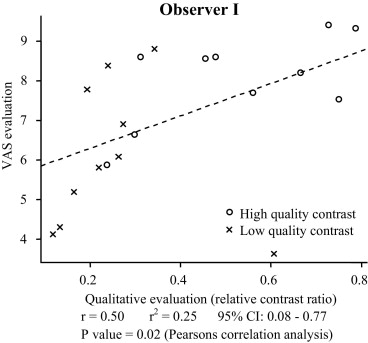
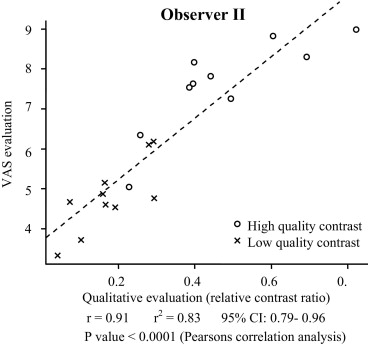
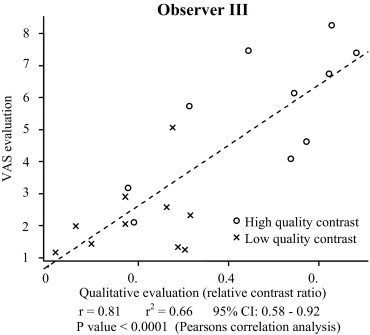
Table 3
Interclass Correlation of Subjective and Qualitative Evaluation
Quantitative Evaluation ⁎ Qualitative Evaluation † ICC ‡ P -value § ICC ‡ P- value § Observer II vs. I 0.74 <.0001 0.83 <.0001 Observer II vs. III 0.85 <.0001 0.89 <.0001
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kronborg O., Fenger C., Olsen J., Jorgensen O.D., Sondergaard O.: Randomised study of screening for colorectal cancer with faecal-occult-blood test. Lancet 1996; 348: pp. 1467-1471.
2. Hardcastle J.D., Chamberlain J.O., Robinson M.H., Moss S.M., Amar S.S., Balfour T.W., et. al.: Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet 1996; 348: pp. 1472-1477.
3. Mandel J.S., Bond J.H., Church T.R., Snover D.C., Bradley G.M., Schuman L.M., et. al.: Reducing mortality from colorectal cancer by screening for fecal occult blood. N Engl J Med 1993; 328: pp. 1365-1371.
4. Lauenstein T., Holtmann G., Schoenfelder D., Bosk S., Ruehm S.G., Debatin J.F.: MR colonography without colonic cleansing: A new strategy to improve patient acceptance. AJR Am J Roentgenol 2001; 177: pp. 823-827.
5. Papanikolaou N., Grammatikakis J., Maris T., Lauenstein T., Prassopoulos P., Gourtsoyiannis N.: MR colonography with fecal tagging: Comparison between 2D turbo FLASH and 3D FLASH sequences. Eur Radiol 2003; 13: pp. 448-452.
6. Saar B., Meining A., Beer A., Settles M., Helmberger H., Frimberger E., et. al.: Prospective study on bright lumen magnetic resonance colonography in comparison with conventional colonoscopy. Br J Radiol 2007; 80: pp. 235-241.
7. Ristvedt S.L., McFarland E.G., Weinstock L.B., Thyssen E.P.: Patient preferences for CT colonography, conventional colonoscopy, and bowel preparation. Am J Gastroenterol 2003; 98: pp. 578-585.
8. Svensson M.H., Svensson E., Lasson A., Hellstrom M.: Patient acceptance of CT colonography and conventional colonoscopy: Prospective comparative study in patients with or suspected of having colorectal disease. Radiology 2002; 222: pp. 337-345.
9. Weishaupt D., Patak M.A., Froehlich J., Ruehm S.G., Debatin J.F.: Faecal tagging to avoid colonic cleansing before MRI colonography. Lancet 1999; 354: pp. 835-836.
10. Ajaj W., Pelster G., Treichel U., Vogt F.M., Debatin J.F., Ruehm S.G., et. al.: Dark lumen magnetic resonance colonography: Comparison with conventional colonoscopy for the detection of colorectal pathology. Gut 2003; 52: pp. 1738-1743.
11. Kuehle C.A., Langhorst J., Ladd S.C., Zoepf T., Nuefer M., Grabellus F., et. al.: Magnetic resonance colonography without bowel cleansing: A prospective cross sectional study in a screening population. Gut 2007; 56: pp. 1079-1085.
12. Goehde S.C., Descher E., Boekstegers A., Lauenstein T., Kuhle C., Ruehm S.G., et. al.: Dark lumen MR colonography based on fecal tagging for detection of colorectal masses: Accuracy and patient acceptance. Abdom Imaging 2005; 30: pp. 576-583.
13. Achiam M.P., Chabanova E., Logager V., Thomsen H.S., Rosenberg J.: Implementation of MR colonography. Abdom Imaging 2007; 32: pp. 457-462.
14. Magnetic Resonance in Medicine: The Basic Textbook of the European Magnetic Resonance Forum.4th ed.2001.Blackwell Wissenschafts-VerlagBerlin/Vienna
15. Pickhardt P.J., Choi J.R., Hwang I., Butler J.A., Puckett M.L., Hildebrandt H.A., et. al.: Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med 2003; 349: pp. 2191-2200.
16. Cotton P.B., Durkalski V.L., Pineau B.C., Palesch Y.Y., Mauldin P.D., Hoffman B., et. al.: Computed tomographic colonography (virtual colonoscopy): A multicenter comparison with standard colonoscopy for detection of colorectal neoplasia. JAMA 2004; 291: pp. 1713-1719.
17. Lauenstein T.C., Debatin J.F.: Magnetic resonance colonography with fecal tagging: An innovative approach without bowel cleansing. Top Magn Reson Imaging 2002; 13: pp. 435-444.