
Rationale and Objectives
To evaluate the long-term clinical outcomes of magnetic resonance–guided high-intensity focused ultrasound (MR-g HIFU) treatments for symptomatic uterine leiomyomata.
Materials and Methods
Patients were recruited for a prospective study for MR-g HIFU treatments of symptomatic leiomyomata, with up to 3-year follow-up. The study was approved by the institutional review board and was Health Insurance Portability and Accountability Act–compliant. Clinical assessments were obtained at 3 months, 6 months, and 1, 2, and 3 years after MR-g HIFU, as well as uterine fibroid symptom severity scores (SSS) and health-related quality of life questionnaires (UFS-QOL). MR imaging was performed at each follow-up to assess the efficacy of the treatment at 6 months, 1 year, 2 years, and 3 years.
Results
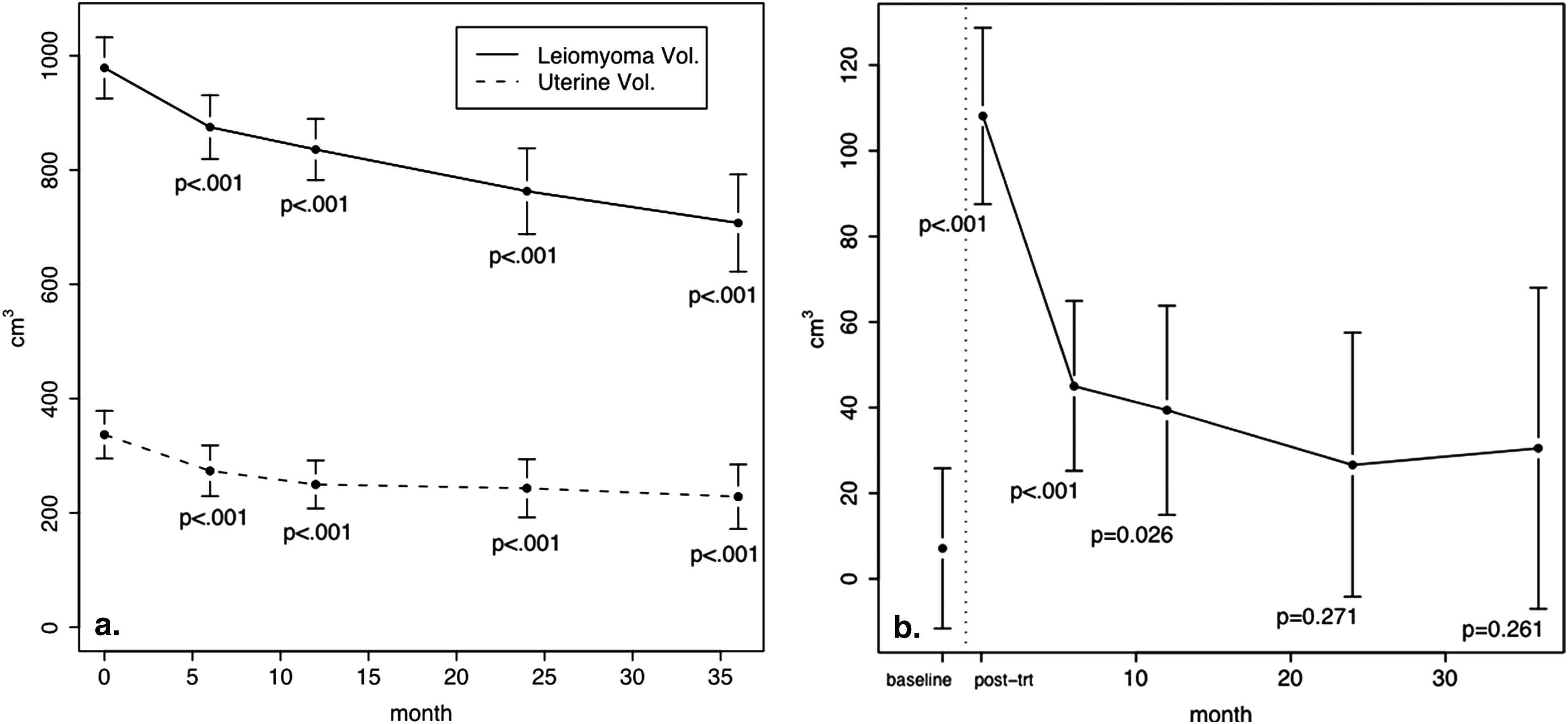
Fifty-one leiomyomata in 40 patients were treated. All patients were treated within the US Food and Drug Administration guidelines with leiomyomata localized on MR and treated with sonication. The mean baseline volume of treated leiomyomata was 336.9 cm 3 . The mean improvement scores for transformed SSS was 47.8 ( P < .001) and for tUFS-QOL was 39.8 ( P < .001) at 3 years. The mean volume decrease in treated leiomyomata was 32.0% ( P < .001), and, in the uterus, the volume decrease was 27.7% ( P < .001) at 3 years. There were no long-term complications.
Conclusions
Long-term follow-up data from MR-g HIFU treatments show sustained symptomatic relief among enrolled patients. Although the results are preliminary, MR-g HIFU for the treatment of uterine leiomyomata may result in acceptable long-term outcomes at 3 years.
Uterine leiomyomata occur in approximately 20%–50% of women of reproductive age . Symptoms are found in less than 50% of women; however, uterine leiomyomata can cause significant morbidity in pre- and perimenopausal women. Traditionally, gold standard therapy has been a hysterectomy. In the United States alone, hysterectomy is performed in more than 600,000 women annually and uterine leiomyomata account for approximately 30%–60% of all hysterectomies performed in middle-age women . More than $1.2 billion is spent each year associated with hysterectomies . The cost is even greater when accounted for the loss of women’s productivity during 6–8 weeks of recovery time after hysterectomy or myomectomy is considered.
Less invasive surgical techniques have been studied. Myomectomy is performed in 35,000–40,000 women for the treatment of uterine leiomyomata . Laparoscopic and hysteroscopic myomectomy have gained popularity as uterus-conserving surgeries . These less invasive techniques are restricted with regard to size and location of leiomyoma and still require general anesthesia. Laparoscopic thermoablative myolysis has shown significant variability in clinical efficacy .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MR-g HIFU Techniques
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MR Imaging Parameters
Get Radiology Tree app to read full this article<
Study Endpoints
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Clinical Assessment: tSSS and tQOL
tSSS tQOL Time Mean Value (95% CI) Mean Change (95% CI) Mean Value (95% CI) Mean Change (95% CI) Baseline 64.8 (59.1–70.6) 44.1 (37.7–50.6) 3 month 35.3 (29.3, 41.3) −29.5 (−37.8, −21.3) 68.8 (62.1–75.6) 24.6 (15.4–34.1) 6 month 32.2 (26.3–38.2) −32.6 (−40.9 to −24.3) 68.6 (61.9–75.4) 24.5 (15.2–33.9) 1 year 40.5 (32.5–48.7) −24.3 (−34.2 to −14.3) 68.7 (59.6–77.9) 24.6 (13.4–35.8) 2 year 18.0 (8.0–28.1) −46.8 (−58.4 to −35.2) 86.1 (74.8–97.5) 42.0 (28.9–51.2) 3 year 17.0 (8.9, 25.1) −47.8 (−57.7, −37.9) 83.9 (74.5–93.3) 39.8 (28.3–51.2)
QOL, quality of life; tQOL, transformed quality of life; tSSS, transformed symptom severity scale.
Table 2
Subgroup Analysis of Uterine Fibroid Symptom - Quality Of Life Questionnaire
Mean Concern Mean Activities Mean Energy Mean Control Mean Consciousness Mean Sexual Function Baseline 47.8 (39.6–56.0) 44.0 (36.3–51.7) 45.4 (38.0–52.8) 45.1 (36.9–53.3) 29.2 (20.2–38.2) 51.1 (42.3–59.8) 3 month 69.4 (60.9–78.0) 68.1 (60.1–76.1) 69.9 (62.2–77.6) 71.8 (63.3–80.4) 59.7 (50.4–69.1) 72.3 (63.2–81.3) 6 month 72.2 (63.6–80.6) 71.0 (63.1–79.0) 71.2 (63.5–78.9) 72.2 (63.6–80.7) 60.1 (50.8–69.5) 75.7 (66.7–84.8) 1 year 71.3 (59.7–82.8) 68.2 (57.4–79.1) 72.5 (62.1–82.9) 73.8 (62.1–85.4) 48.8 (36.1–61.5) 68.1 (55.7–80.5) 2 year 90.8 (76.4–105.1) 82.3 (75.9–102.7) 89.6 (76.7–102.5) 86.5 (72.1–100.9) 62.8 (47.0–78.6) 85.6 (70.2–100.9) 3 year 87.4 (75.5–99.2) 82.9 (71.8–94.0) 85.3 (74.6–96.1) 87.4 (75.5–99.3) 69.3 (56.2–82.4) 86.8 (74.1–99.5)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Volume Changes in Leiomyomata, Uterus, and Nonperfused Area within the Treatment Zone
Time Leiomyoma Volume (cm 3 ) Uterine Volume (cm 3 ) Nonperfused Leiomyoma Volume (cm 3 ) Mean Value (95% CI) Mean Change (95% CI), % Change Mean Value
(95% CI) Mean Change
(95% CI), % Change Mean Value
(95% CI) Mean Change
(95% CI), % Change Baseline 336.9 (295.2–378.6) 978.7 (925.1–1032.3) 7.1
(−11.6 to 25.8), 2.1% Immediate posttreatment 108.1 (87.5–128.7), 32.1% 101.0 (76.6–125.5),
1422.5% 6 month 273.6 (229.3–318.0) −63.3 (−96.5 to −30.0), −18.7% 875.0 (819.2–930.8) −103.7 (−159.4 to −47.9), −10.5% 45.0 (25.2–64.9), 16.5% 40.0 (14.1–61.9),
563.4% 1 year 249.7 (207.7–291.7) −87.2 (−127.7 to −46.7), −25.8% 835.9 (782.4–889.5) −142.7 (−209.8 to −75.7), −14.5% 39.4 (14.9–63.8), 15.8% 32.3 (3.9–60.7),
454.9% 2 year 243.1 (192.2, 293.9) −93.9 (−142.5 to −45.2), −27.6% 762.9 (687.9–837.9) −215.7 (−296.4 to −135.1), −22.0% 26.6 (−4.2 to 57.5), 10.9% 19.6(−15.2 to 54.4),
276.1% 3 year 228.4 (171.9–284.8) −108.5 (165.5 to −51.4), −32.0% 707.3 (622.2–792.4) −271.4 (−365.1 to −177.7), −27.7% 30.5 (−7.0 to 68.0), 13.4% 23.4 (−17.5 to 64.3),
329.6%
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Buttram V.C.J., Reiter R.C.: Uterine leiomyomata: etiology, symptomatology, and management. Fertil Steril 1981; 36: pp. 433-445.
2. Vollenhoven B.J., Lawrence A.S., Healy D.L.: Uterine fibroids: a clinical review. Br J Obstet Gynaecol 1990; 97: pp. 285-298.
3. Bernstein S.J., Fiske M.E., McGlynn E.A., et. al.: Hysterectomy: a review of the literature on indications, effectiveness, and risks.1998.RandSanta Monica, CA
4. Lepine L., Hillis S., Marchbanks P., et. al.: Hysterectomy surveillance—United States, 1980–1993. MMWR CDC Surveill Summ 1997; 46: pp. 1-15.
5. Xhao S., Wong J., Arguelles L.: Hospitalization costs associated with leiomyoma. Clin Ther 1999; 21: pp. 563-575.
6. National Center for Health Statistics: Ambulatory and Inpatient Procedures in the United States. DHHS Publication No. (PHS) 99-1710 1998;
7. Stewart E.: Uterine fibroids. Lancet 2001; 357: pp. 293.
8. Goldfarb H.: Myoma coagulation (myolysis). Obstet Gynecol Clin North Am 2000; 27: pp. 421-430.
9. Zreik T., Rutherford T., Palter S., et. al.: Cryomyolysis, a new procedure for the conservative treatment of uterine fibroids. J Am Assoc Gynecol Laparosc 1998; 5: pp. 33-38.
10. Spies J.B., Ascher S.A., Roth A.R., et. al.: Uterine artery embolization for leiomyomata. Obstet Gynecol 2001; 98: pp. 29-34.
11. Spies J.B., Myers E.R., Worthington-Kirsch R., et. al.: The FIBROID Registry: symptom and quality-of-life status 1 year after therapy. Obstet Gynecol 2005; 106: pp. 1309-1318.
12. Pron G., Bennett J., Common A., et. al.: Technical results and effects of operator experience on uterine artery embolization for fibroids: the Ontario Uterine Fibroid Embolization Trial. J Vasc Interv Radiol 2003; 14: pp. 545-554.
13. Pron G., Mocarski E., Bennett J., et. al.: Tolerance, hospital stay, and recovery after uterine artery embolization for fibroids: the Ontario Uterine Fibroid Embolization Trial. J Vasc Interv Radiol 2003; 14: pp. 1243-1250.
14. Spies J.B., Spector A., Roth A.R., et. al.: Complications after uterine artery embolization for leiomyomas. Obstet Gynecol 2002; 100: pp. 873-880.
15. Kim H.S., Thonse V.R., Judson K., et. al.: Utero-ovarian anastomosis—histopathologic correlation after uterine artery embolization with or without ovarian artery embolization. J Vasc Interv Radiol 2007; 18: pp. 31-39.
16. Kim H.S., Tsai J., Lee J.M., et. al.: Effects of utero-ovarian anastomoses on basal follicle-stimulating hormone level change after uterine artery embolization with tris-acryl gelatin Microspheres. J Vasc Interv Radiol 2006; 17: pp. 965-971.
17. Kim H.S., Tsai J., Jacobs M.A., et. al.: Percutaneous image-guided radiofrequency thermal ablation for large symptomatic uterine leiomyomata after uterine artery embolization: a feasibility and safety study. J Vasc Interv Radiol 2007; 18: pp. 41-48.
18. Cowan B., Sewell P., Howard J., et. al.: Interventional magnetic resonance imaging cryotherapy of uterine fibroid tumors: preliminary observation. Am J Obstet Gynecol 2002; 186: pp. 1183.
19. Sakuhara Y., Shimizu T., Kodama Y., et. al.: Magnetic resonance-guided percutaneous cryoablation of uterine fibroids: early clinical experiences. Cardiovasc Intervent Radiol 2006; 29: pp. 552-558.
20. Hindley J.T., Law P.A., Hickey M., et. al.: Clinical outcomes following percutaneous magnetic resonance image guided laser ablation of symptomatic uterine fibroids. Hum. Reprod 2002; 17: pp. 2737-2741.
21. Hindley J., Gedroyc W.M., Regan L., et. al.: MRI guidance of focused ultrasound therapy of uterine fibroids: early results. Am J Roentgenol 2004; 183: pp. 1713-1719.
22. Jacobs M.A., Herskovits E.H., Kim H.S.: Uterine fibroids: diffusion-weighted MR imaging for monitoring therapy with focused ultrasound surgery—preliminary study. Radiology 2005; 236: pp. 196-203.
23. Stewart E.A., Gostout B., Rabinovici J., et. al.: Sustained relief of leiomyoma symptoms by using focused ultrasound surgery. Obstet Gynecol 2007; 110: pp. 279-287.
24. Stewart E.A., Rabinovici J., Tempany C.M., et. al.: Clinical outcomes of focused ultrasound surgery for the treatment of uterine fibroids. Fertil Steril 2006; 85: pp. 22-29.
25. Zowall H., Cairns J.A., Brewer C., et. al.: Cost-effectiveness of magnetic resonance-guided focused ultrasound surgery for treatment of uterine fibroids. BJOG Int J Obstet Gynaecol 2008; 115: pp. 653-662.
26. Spies J.B., Coyne K., Guaou N.G., et. al.: The UFS-QOL, a new disease-specific symptom and health-related quality of life questionnaire for leiomyomata. Obstet Gynecol 2002; 99: pp. 290-300.
27. Goodwin S.C., Bonilla S.C., Sacks D., et. al.: Reporting standards for uterine artery embolization for the treatment of uterine leiomyomata. J Vasc Interv Radiol 2003; 14: pp. 467-476.
28. Diggle P., Heagerty P., Liang K.-Y., et. al.: Analysis of longitudinal data.2002.Oxford University Press2nd ed. Oxford, UK
29. Goodwin S.C., Spies J.B., Worthington-Kirsch R., et. al.: Uterine artery embolization for treatment of leiomyomata: long-term outcomes from the FIBROID Registry. Obstet Gynecol 2008; 111: pp. 22-33.
30. Kim H.S., Paxton B.E., Lee J.M.: Long-term efficacy and safety of uterine artery embolization in young patients with and without uteroovarian anastomoses. J Vasc Interv Radiol 2008; 19: pp. 195-200.
31. Spies J.B., Bruno J., Czeyda-Pommersheim F., et. al.: Long-term outcome of uterine artery embolization of leiomyomata. Obstet Gynecol 2005; 106: pp. 933-939.
32. Banovac F., Ascher S.M., Jones D.A., et. al.: Magnetic resonance imaging outcome after uterine artery embolization for leiomyomata with use of tris-acryl gelatin microspheres. J Vasc Interv Radiol 2002; 13: pp. 681-688.
33. Kim H.S., Tsai J., Patra A., et. al.: Effects of utero-ovarian anastomoses on clinical outcomes and repeat intervention rates after uterine artery embolization. J Vasc Interv Radiol 2006; 17: pp. 783-789.
34. Pelage J.P., Guaou N.G., Jha R.C., et. al.: Uterine fibroid tumors: long-term MR imaging outcome after embolization. Radiology 2004; 230: pp. 803-809.