
Rationale and Objectives
To identify magnetic resonance (MR) imaging characteristics allowing specific preoperative discrimination between colloid cysts (CCs) of the sellar region and third ventricle (CC3rdv) versus Rathke’s cleft cysts (RCCs).
Materials and Methods
MR imaging data of 38 patients with histologically proven CCs/CC3rdv and RCC underwent retrospective analysis with respect to signal intensity and heterogeneity on T1- and T2-weighted images, presence of the dot sign, enhancement, size, location, and accompanying infundibular stalk abnormalities.
Results
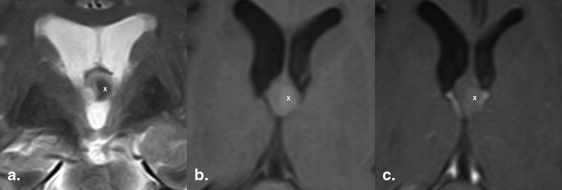
Thirteen patients had CCs, 12 had CC3rdv, and 13 had RCCs. Signal intensity on T1-weighted images was partly or entirely hyperintense ( n = 8), iso- or mixed iso/hypointense ( n = 5) in CCs; hyperintense ( n = 8), isointense, or mixed hypo/isointense ( n = 3) in CC3rdv and hyperintense ( n = 9); or mixed ( n = 4) in RCCs. On T2-weighted images, signal intensity was hypointense ( n = 12) or hyperintense ( n = 1) in CCs, hypointense ( n = 9) or hyperintense ( n = 2) in CC3rdv, and hypointense ( n = 5) or iso/hyperintense ( n = 8) in RCCs. T2-weighted images were unavailable in two patients. Only one questionable enhancement was found in CCs, whereas an enhancing rim was consistently seen in RCCs. The dot sign was present in 7 CCs, 8 CC3rdv, and 4 RCCs. Mean cyst diameters were 12.6 mm for CCs and 14.5 mm for RCCs. RCCs showed more frequent and even solely suprasellar extent contrary to CCs.
Conclusion
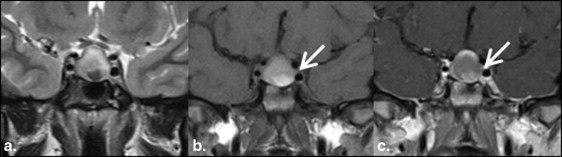
Cyst wall enhancement was found in all RCCs but in none of the CCs, making this feature a reliable discriminator between the two. Complementary, suprasellar extension was more frequent in RCCs, whereas signal hypointensity on T2w was more common in colloid cysts.
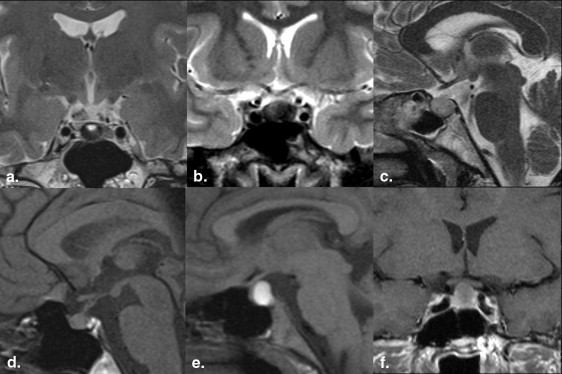
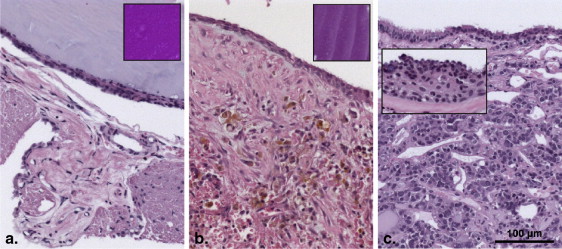
Colloid cysts (CC) are benign, epithelial-lined mass lesions occurring in different locations, mostly attached to the anterosuperior aspect of the third ventricle between the columns of the fornices. Imaging features of CC of the third ventricle (CC3rdv) have already been reported and, because of their typical location, the spectrum of differential diagnoses is fairly restricted. Their magnetic resonance (MR) signal characteristics are dependent on the composition of the cyst content, in which T1-weighted signal correlates with cholesterol concentration (2/3 of them being hyperintense on nonenhanced T1-weighted images), whereas T2-weighted signal is variable. The latter reflects either water content (mostly isointense to the brain) or small amounts of paramagnetic substances contained in macrophages within CC (usually hypointense to the brain). Moreover, CC contain dense material of variable viscosity (mucoid or desiccated) intermixed with old blood, hemosiderin, cholesterol crystals, and various ions that seriously impact the MR signal. CC show no enhancement, not even in the cyst wall . The lining of CC3rdv is variable with stretches of cuboidal or flattened columnar epithelium that may alter with simple or pseudostratified epithelium.
Contrary to CC3rdv, the spectrum of differentials in case of CC of the sellar region (CCs) is more challenging. CCs are located between the anterior and posterior lobe of the pituitary gland and represent part of the so-called pars intermedia masses. Discrimination from other predominantly or entirely cystic masses such as Rathke’s cleft cysts (RCCs), arachnoid cysts, cystic adenomas, craniopharyngiomas, empty sella, pituitary necrosis, or some types of hypophysitis often proves difficult.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Material and methods
Patient Characteristics
Get Radiology Tree app to read full this article<
Imaging
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Histologic Analysis
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Demographics of Patients with CCs and RCCs
Get Radiology Tree app to read full this article<
Clinical Presentation of Patients with CCs and RCCs
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MR Imaging Characteristics in CCs
Get Radiology Tree app to read full this article<
Table 1
Magnetic Resonance Signal Characteristics in Patients with Colloid Cyst of the Sellar Region and Presence of Cyst Wall and Inflammation Within Cyst Wall in the Histology
Age Gender T1-weighted Hyperintense T2-weighted Hypointense FLAIR = T2 T1-weighted CE Mixed Signal Localization Cyst Wall Inflammation 50 F + + + +? + I + S + 0 48 F + + + 0 + I + S + 0 39 F 0 0 + 0 0 I + 0 30 M + + + 0 + I + 0 28 F 0 + + 0 0 I + S + 0 29 F + + + 0 0 I 0 0 27 F + + + 0 0 I + 0 27 F 0 + + 0 + I 0 0 18 M + + + 0 + I + 0 19 F + + + 0 0 I + S 0 0 12 F 0 + + 0 0 I + S 0 0 9 M 0 + NA 0 + I 0 0 23 F + + + 0 + I + S 0 0
0, not present; +, present; CE, contrast enhancement; cyst wall, presence of an identifiable cyst wall on magnetic resonance imaging; I, intrasellar; NA, no image available; S, suprasellar.

Get Radiology Tree app to read full this article<
MR Imaging Characteristics in CC3rdv
Get Radiology Tree app to read full this article<
Table 2
Magnetic Resonance Signal Characteristics in Patients with Colloid Cysts of the Third Ventricle and Presence of Cyst Wall and Inflammation Within Cyst Wall in the Histology
Age Gender T1-weighted Hyperintense T2-weighted Hypointense FLAIR = T2 T1-weighted CE Mixed Signal Cyst Wall Inflammation 56 M + + + NA + + 0 47 F NA + + NA + 0 0 40 F + NA NA 0 0 0 0 42 M + + + 0 0 + 0 45 M + + + 0 + + 0 38 F + + NA NA + + 0 31 M 0 0 + NA 0 + 0 31 F + + + 0 + 0 0 30 M + + + 0 + 0 0 59 M 0 + + 0 + + 0 32 F + + + 0 + 0 0 27 M 0 0 + 0 0 + 0
0, not present; +, present; CE, contrast enhancement; cyst wall, presence of an identifiable cyst wall on magnetic resonance imaging; NA, no image available.
Get Radiology Tree app to read full this article<
MR Imaging Characteristics in RCCs
Get Radiology Tree app to read full this article<
Table 3
Magnetic Resonance Signal Characteristics in Patients with Rathke Cleft Cysts and Presence of Cyst Wall and Inflammation Within Cyst Wall in the Histology
Age Gender T1-weighted Hyperintense T2-weighted Hypointense FLAIR = T2 T1-weighted CE Mixed Signal Localization Cyst Wall Inflammation 46 F + 0 + + 0 S + 0 52 F + + + + 0 I + S + + 56 F + + + + + I + S + 0 55 F 0 0 + + 0 I + S + 0 17 F 0 0 + + 0 I + S + + 46 M + 0 NA + 0 I + S + 0 68 M + 0 + + + S + + 21 F + + + + + I + S + + 45 F 0 0 + + 0 I + S + 0 32 F + 0 + + 0 I + + 14 F + + + + + I + S + P + + 46 F 0 0 + + 0 S + I + 0 57 M + + + + + S + I + +
Enhancement was in all cases seen at the rim of the cyst.
0, not present; +, present; CE, contrast enhancement; cyst wall, presence of an identifiable cyst wall on magnetic resonance imaging; I, intrasellar; NA, no image available; S, suprasellar.

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Histological Characteristics of CC and RCCs
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Nomikos P., Buchfelder M., Fahlbusch R.: Intra- and suprasellar colloid cysts. Pituitary 1999; 2: pp. 123-126.
2. Teramoto A., Hirakawa K., Sanno N., et. al.: Incidental pituitary lesions in 1,000 unselected autopsy specimens. Radiology 1994; 193: pp. 161-164.
3. Kuchelmeister K., Bergmann M.: Colloid cysts of the third ventricle: an immunohistochemical study. Histopathology 1992; 21: pp. 35-42.
4. Saeger W.: Space occupying processes of the sellar region with emphasis on tumor-like lesions. Pathologe 2003; 24: pp. 247-254.
5. Nishioka H., Haraoka J., Izawa H., et. al.: Magnetic resonance imaging, clinical manifestations, and management of Rathke’s cleft cyst. Clin Endocrinol (Oxf) 2006; 64: pp. 184-188.
6. Müller H.L., Gebhardt U., Faldum A., et. al.: Xanthogranuloma, Rathke’s cyst, and childhood craniopharyngioma: results of prospective multinational studies of children and adolescents with rare sellar malformations. J Clin Endocrinol Metab 2012; 97: pp. 3935-3943.
7. Bladowska J., Bednarek-Tupikowska G., Biel A., et. al.: Colloid cyst of the pituitary gland: case report and literature review. Pol J Radio 2010; 75: pp. 88-93.
8. Graziani N., Dufour H., Figarella-Branger D., et. al.: Do the suprasellar neurenteric cyst, the Rathke cleft cyst and the colloid cyst constitute a same entity?. Acta Neurochir (Wien) 1995; 133: pp. 174-180.
9. Zielinski G., Podgorski J.K., Siwik J., et. al.: Colloid cysts of the pituitary gland. Neurol Neurochir Pol 2002; 36: pp. 293-306.
10. Armao D., Castillo M., Chen H., et. al.: Colloid cyst of the third ventricle: imaging-pathologic correlation. AJNR Am J Neuroradiol 2000; 21: pp. 1470-1477.
11. Algin O., Ozmen E., Arslan H.: Radiologic manifestations of colloid cysts: a pictorial essay. Can Assoc Radiol J 2013; 64: pp. 56-60.
12. Alnaghmoosh N., Alkhani A.: Colloid cysts in children, a clinical and radiological study. Childs Nerv Sys 2006; 22: pp. 514-516.
13. Algin O., Ozmen E., Arslan H.: Radiologic manifestations of colloid cysts: a pictorial essay. Can Assoc Radiol J 2013; 64: pp. 56-60.
14. Scotti G., Scialfa G., Colombo N., et. al.: MRI in the diagnosis of colloid cysts of the third ventricle. AJNR Am J Neuroradiol 1987; 8: pp. 370-372.
15. Shin J.L., Asa S.L., Woodhouse L.J., et. al.: Cystic lesions of the pituitary: clinicopathological features distinguishing craniopharyngioma, Rathke’s cleft cyst, and arachnoid cyst. J Clin Endocrinol Metab 1999; 84: pp. 3972-3982.
16. Kim E.: A case of ectopic Rathke’s cleft cyst in the prepontine cistern. J Korean Neurosurg Soc 2012; 52: pp. 152-155.
17. Brassier G., Morandi X., Tayiar E., et. al.: Rathke’s cleft cysts: surgical-MRI correlation in 16 symptomatic cases. J Neuroradiol 1999; 26: pp. 162-171.
18. Aho C.J., Liu C., Zelman V., et. al.: Surgical outcomes in 118 patients with Rathke cleft cysts. J Neurosurg 2005; 102: pp. 189-193.
19. Kim J.E., Kim J.H., Kim O.L., et. al.: Surgical treatment of symptomatic Rathke cleft cysts: clinical features and results with special attention to recurrence. J Neurosurg 2004; 100: pp. 33-40.
20. Wolfsohn A.L., Lach B., Benoit B.G.: Suprasellar xanthomatous Rathke’s cleft cyst. Surg Neurol 1992; 38: pp. 106-109.
21. Itoh J., Usui K.: An entirely suprasellar symptomatic Rathke’s cleft cyst: case report. Neurosurgery 1992; 30: pp. 581-594.
22. Wang S.S., Xiao D.Y., Yu Y.H., et. al.: Diagnostic significance of intracystic nodules on MRI in Rathke’s cleft cyst. Int J Endocrinol 2012; 2012: pp. 958732.
23. Cohan P., Foulad A., Esposito F., et. al.: Symptomatic Rathke’s cleft cysts: a report of 24 cases. J Endocrinol Invest 2004; 27: pp. 943-948.
24. Frank G., Sciarretta V., Mazzatenta D., et. al.: Transsphenoidal endoscopic approach in the treatment of Rathke’s cleft cyst. Neurosurgery 2005; 56: pp. 124-128.
25. Cavallo L.M., Prevedello D., Esposito F., et. al.: The role of the endoscope in the transsphenoidal management of cystic lesions of the sellar region. Neurosurg Rev 2008; 31: pp. 55-64.
26. Honegger J., Fahlbusch R., Bornemann A., et. al.: Lymphocytic and granulomatous hypophysitis: experience with nine cases. Neurosurgery 1997; 40: pp. 713-723.
27. Ogawa Y., Tominaga T.: A partially ossified solid and cystic Rathke cleft cyst. J Neurosurg 2010; 112: pp. 1324-1326.
28. Wolfe S.Q., Heros R.C.: A Rathke cleft cyst to craniopharyngioma: is there a spectrum?. J Neurosurg 2010; 112: pp. 1322-1323.