
Rationale and Objectives
Conventional tractography based on the “streamline” method only partially visualizes the pyramidal tract because of fiber crossing with other white matter tracts. Recently a new tractography method based on directional diffusion function (DDF) has been proposed. This method was reported to visualize the pyramidal tract to a larger extent than conventional techniques do. To validate the DDF-based tractography method, we studied the somatotopic organization of the pyramidal tract in the posterior limb of the internal capsule (PLIC).
Materials and Methods
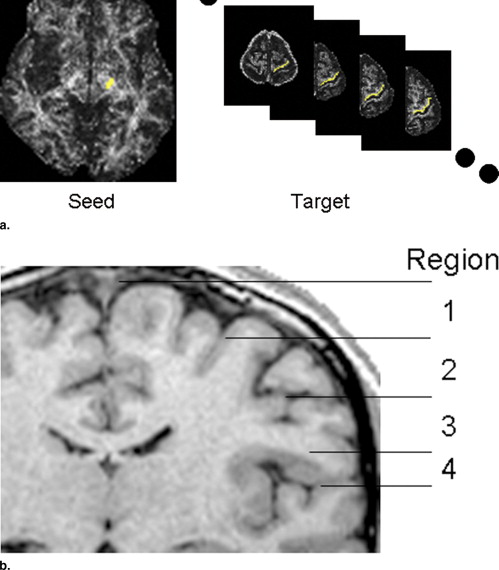
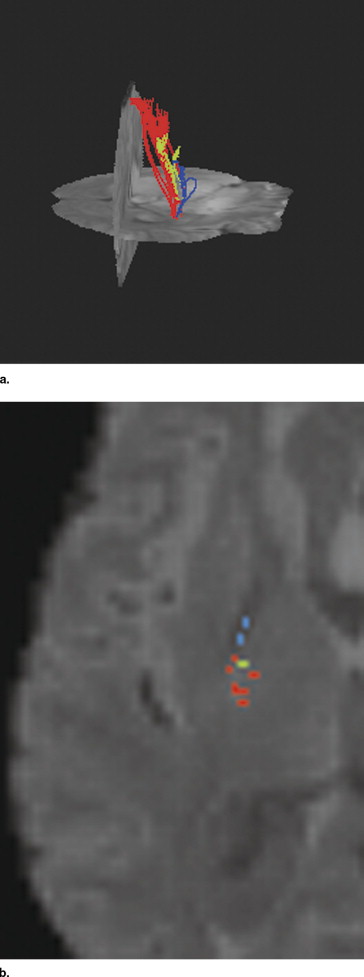
Pyramidal tracts in the intact hemispheres of 14 brain tumor patients were drawn using the directional diffusion function-based tractography method. Each pyramidal tract was divided into four fiber bundles according to the cephalocaudal positions of their termination in the precentral gyrus. The cephalocaudal positions in the precentral gyrus of the four fiber bundles were correlated with their positional relationships in the PLIC along the mediolateral and anteroposterior axes.
Results
Fiber bundles terminating more caudally in the precentral gyrus were located significantly more anteriorly in the PLIC ( r = 0.59, Spearman’s correlation coefficient, P < .0001). On the other hand, no significant correlation was shown between the cephalocaudal positions in the precentral gyrus of the four fiber bundles and their relative positions in the PLIC along the mediolateral axis.
Conclusions
Estimated organization of the fiber bundles of the pyramidal tract in the PLIC was consistent with anatomically known somatotopic organization, which supported the validity of the DDF-based tractography method.
Magnetic resonance (MR) tractography is an image processing method to visualize the white matter tract in the brain based on diffusion tensor imaging (DTI) data ( ). The efficacy of this emerging technique has recently been investigated in several clinical applications, including preoperative and intraoperative surgical planning for brain tumors ( ). Visualization of the pyramidal tract (PT), the most eloquent white matter tract, using tractography, is expected to help avoid accidental damage to this white matter tract during brain surgery. Tractography is still a relatively new technique, however, and needs further technical improvements. Most important, current tractography, which is based on the “streamline” technique ( ), may be significantly affected by crossing with other white matter tracts. In this technique, fibers within the white matter tract are traced along the principal eigenvector of local diffusion tensor. In estimating PT, crossing with the superior longitudinal fasciculus and fibers emerging from the corpus callosum interferes with the local diffusion tensor, rendering the affected fibers untraceable. As a result, with the conventional tractography, the PT is visualized only partially. This problem is important because the invisible part of the PT can be accidentally damaged during the surgical procedure.
Recently, a novel tractography method was proposed by Kumazawa et al that enables visualization of the PT to a larger extent than is allowed by conventional techniques ( ). This new technique is based on the three-dimensional (3D) directional diffusion function (DDF), which is defined by a 3D probability function of the local diffusion tensor. The PT drawn with this new method appears reasonable to visual inspection ( ), yet needs further validation based on objective criteria. As a first step toward the full validation, we investigated somatotopic organization of the PT in the posterior limb of the internal capsule (PLIC) using the DDF-based tractography method, and we compared the results with known anatomical relationships. It is well established that there is homuncular organization in the primary motor cortex ( ), which is located in the precentral gyrus (PRCG). Motor functions in face, hand, and lower trunk/buttock are controlled by the caudal, middle, and cephalad portions of the motor cortex, respectively. The foot motor area is located in the medial continuation of the motor cortex. Somatotopic organization of the neuronal fibers in the PT, which mainly consists of axonal fibers from the primary motor cortex, has been previously investigated by an electrophysiologic method ( ), and the general consensus is that fibers from the face, hand, and foot motor areas are arranged from anterior to posterior in the PLIC, although their exact locations in the PLIC have been still controversial ( ). In other words, fibers from the caudal PRCG are located more anteriorly, while those from the cephalad PRCG are more posteriorly. We studied PTs using the DDF-based tractography and examined whether the estimated PTs shows such a positional relationship in the PLIC.
Materials and methods
Subjects
Get Radiology Tree app to read full this article<
MR Image Acquisition
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
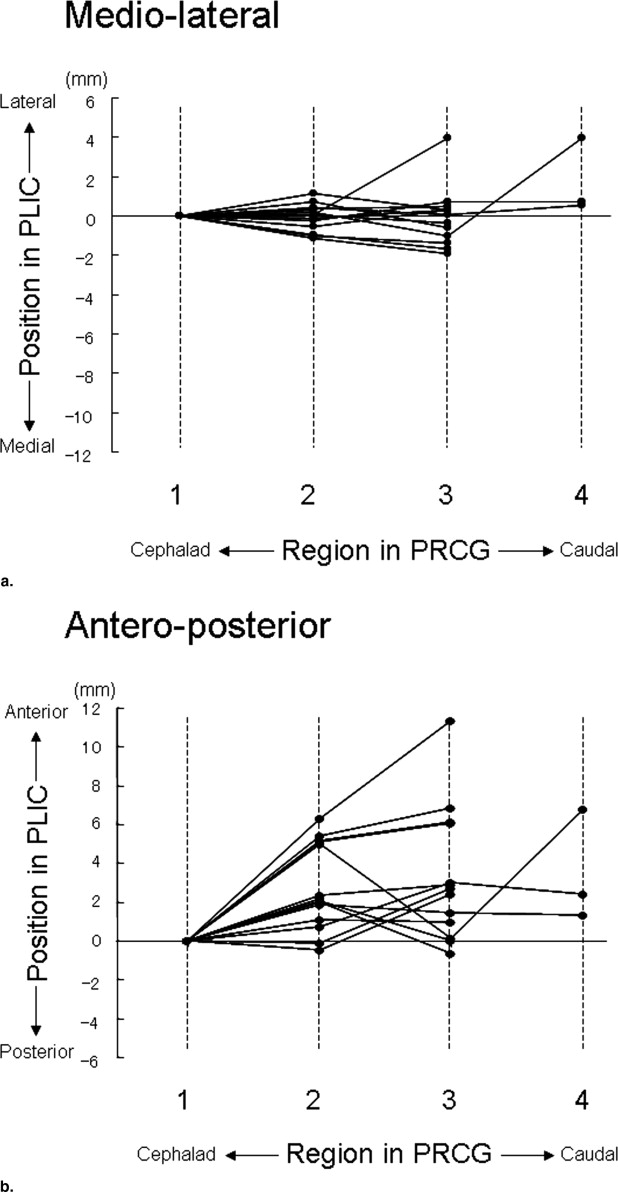
Table 1
Depiction Rate of 4-Fiber Bundles and Relative Positions of Fiber Bundles 2, 3, and 4 (mean ± SD) Indicated in Relation to the Position of Fiber Bundle 1
Fiber Bundle 1 2 3 4 Depiction rate (%) 100 (14/14) 100 (14/14) 92.9 (13/14) 23.1 (3/14) Mediolateral (mm) 0 0 ± 0.7 0.1 ± 1.5 1.7 ± 1.9 Anteroposterior (mm) 0 2.8 ± 2.2 ⁎ 3.3 ± 3.4 ⁎ 3.5 ± 2.9
Positive values indicate lateral and anterior positions to the reference along the mediolateral and anteroposterior axes.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Conturo T.E., Lori N.F., Cull T.F., et. al.: Tracking neuronal fiber pathways in the living human brain. Proc Natl Acad Sci U S A 1999; 96: pp. 10422-10427.
2. Mori S., Crain B.J., Chacko V.P., et. al.: Three-dimensional tracking of axonal projections in the brain by magnetic resonance imaging. Ann Neurol 1999; 45: pp. 265-269.
3. Basser P.J., Pajevic S., Pierpaoli C., et. al.: In vivo fiber tractography using DT-MRI data. Magn Reson Med 2000; 44: pp. 625-632.
4. Mori S., Frederiksen K., van Zijl P.C., et. al.: Brain white matter anatomy of tumor patients evaluated with diffusion tensor imaging. Ann Neurol 2002; 51: pp. 377-380.
5. Kamada K., Todo T., Masutani Y., et. al.: Combined use of tractography-integrated functional neuronavigation and direct nerve stimulation. J Neurosurg 2005; 102: pp. 664-672.
6. Masutani Y., Aoki S., Abe O., et. al.: MR diffusion tensor imaging: recent advance and new techniques for diffusion tensor visualization. Eur J Radiol 2003; 46: pp. 53-66.
7. Kumazawa S., Yoshiura T., Arimura H., et. al.: White matter fiber tractography based on a directional diffusion field in diffusion tensor MRI. Proc SPIE 2006; 6144: pp. 1260-1267.
8. Kumazawa S., Yoshiura T., Arimura H., et. al.: Estimation of white matter connectivity based on a three-dimensional directional diffusion function in diffusion tensor MRI. Med Phys 2006; 33: pp. 4635-4642.
9. Penfield W.G., Boldrey E.: Somatic motor and sensory representation in the cerebral cortex of man as studied by electrical stimulation. Brain 1937; 60: pp. 389-443.
10. Bertrand G., Blundell J., Musella R.: Electrical exploration of the internal capsule and neighboring structures during stereotaxic procedures. J Neurosurg 1965; 22: pp. 333-343.
11. Holodny A.I., Gor D.M., Watts R., et. al.: Diffusion-tensor MR tractography of somatotopic organization of corticospinal tracts in the internal capsule: initial anatomic results in contradistinction to prior reports. Radiology 2005; 234: pp. 649-653.
12. Carpenter M.B.: Human neuroanatomy, ed 8.1983.Williams & WilkinsBaltimore, MD:pp. 537-538.