
Rationale and Objectives
To evaluate breast cancer screening with mammography and magnetic resonance imaging (MRI) in high-risk populations, including women with the BRCA mutation, using an evidence-based approach.
Methods
The MEDLINE, PubMed, EBM Reviews, ACP Journal Club, Cochrane Database MEDSEARCH, and SCOPUS databases were accessed and searched for articles up to August 2007. Articles were collected using the following terms and medical subject headings (MeSH) that applied to the focused clinical question: “BRCA1” and “BRCA2” with “mammography,” “MRI,” “prevention,” “screening,” and “surveillance.” References from retrieved articles were also used to identify relevant papers. Abstracts were screened and relevant papers retrieved. Retrieved papers were graded for quality. Summary performance measures were obtained by random effects modeling of study-specific performance estimates and standard errors derived from the multiple 2 × 2 tables. Additionally, studies meeting the Centre for Evidence-Based Medicine level 2b quality were reviewed.
Results
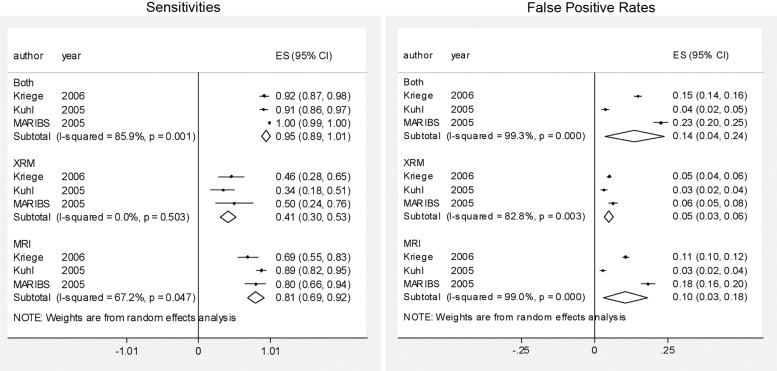
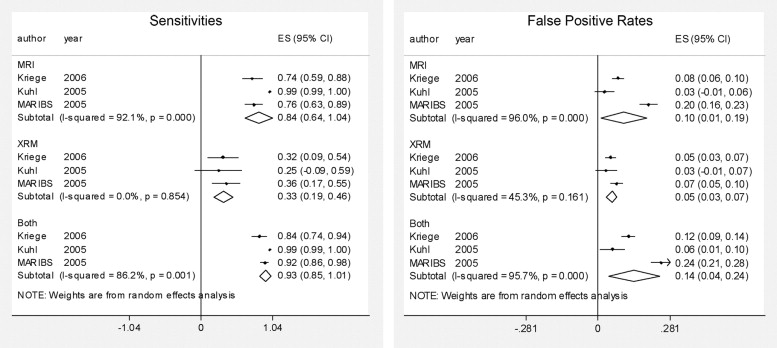
In women with an increased risk without the BRCA gene, cancer detection rates by MRI were 0.011 (95% confidence interval [CI] 0.003–0.019), by mammography 0.005 (95% CI 0.002–0.008), and by a combination of both, 0.012 (95% CI 0.004–0.020). False-positive rates by MRI, mammography, or a combination of both were 0.10 (95% CI 0.03–0.18), 0.05 (95% CI 0.03–0.06), and 0.14 (95% CI 0.04–0.24). In BRCA positive women, cancer detection rates by MRI were 0.027 (95% CI 0.015–0.040), by mammography 0.010 (95% CI 0.005–0.016), and by a combination of both 0.031 (95% CI 0.018–0.045). False-positive rates by MRI, mammography, or a combination of both were 0.10 (95% CI 0.01–0.19), 0.05 (95% CI 0.03–0.07), and 0.14 (95% CI 0.04–0.24), respectively.
Conclusions
The data support an essential role for screening MRI in women with an increased risk for breast cancer.
The most recent American Cancer Society guidelines for breast cancer screening recommend magnetic resonance imaging (MRI) surveillance for women with a 20%–25% or greater lifetime risk of breast cancer ( ). These guidelines do not risk stratify their recommendations based on whether women are BRCA1 or BRCA2 (hereafter collectively referred to as BRCA 1/2) mutational carriers. We used an evidence-based approach to examine the evidence for breast cancer screening with mammography and MRI in the high-risk population, including women carrying the BRCA 1/2 mutation. The evidence-based practice question format Patient, Investigation, Comparison, and Outcomes of interest (PICO) ( ) was used to construct the following focused clinical question: In asymptomatic women at increased risk of breast cancer (BRCA 1/2 mutation carriers or strong family histories), how does MRI compare to mammography and the combination of MRI plus mammography in the detection of benign versus malignant lesions?
Materials and methods
The MEDLINE, PubMed, EBM Reviews, ACP Journal Club, Cochrane Database MEDSEARCH, and SCOPUS databases were accessed and searched for articles up to August 2007. Articles were collected using the following terms and medical subject headings (MeSH) that applied to the focused clinical question: “BRCA1” and “BRCA2” with “mammography,” “MRI,” “prevention,” “screening,” and “surveillance.” References from retrieved articles were also used to identify relevant papers.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Breast Cancer Screening with Magnetic Resonance Imaging in High-risk Women: Study Level Data
Study CEBM Level of Evidence Population Number of Women Screening Events Sens (%) Spec (%) PPV (%) Cancer Detection Rate (%) MARIBS ( ) 2b Family history without BRCA mutation 424 1231 80 81 3 0.7 BRCA 1/2 positive 225 615 76 80 14 3.1 BRCA 1 positive 139 375 92 79 14 3 BRCA 2 positive 86 240 58 82 15 3 Kuhl ( ) 2b Family history without BRCA mutation 486 1033 100 98 52 2.5 BRCA 1/2 positive 43 167 100 98 67 4.8 Kriege ( ) 2b Family history without BRCA mutation 1450 3409 69 89 5 0.5 BRCA 1/2 positive 329 725 74 92 20 1.9 Stoutjesdijk ( ) 3b All women ⁎ 179 258 100 93 43 5.0 Lehman ( ) 3b All women ⁎ 367 367 100 NR 17 1.1 Lehman ( ) 3b All women ⁎ 171 171 100 NR 15 3.5 Warner ( ) 4 All women ⁎ 196 196 86 91 26 3.1 Warner ( ) 4 BRCA 1/2 positive 236 457 77 95 46 3.7
CEBM, Center for Evidence-Based Medicine; NR, not reported; PPV, positive predictive value; Sens, sensitivity; Spec, specificity.
Get Radiology Tree app to read full this article<
Table 2
Breast Cancer Screening with Mammography in High-risk Women: Study Level Data
Study CEBM Level of Evidence Population Number of Women Screening Events Sens (%) Spec (%) PPV (%) Cancer Detection Rate (%) MARIBS ( ) 2b Family history without BRCA mutation 424 1147 50 93 6 0.4 BRCA 1/2 positive 225 617 36 94 17 1.5 BRCA 1 positive 139 388 23 92 9 0.8 BRCA 2 positive 86 229 50 94 32 2.6 Kuhl ( ) 2b Family history without BRCA mutation 486 1033 31 97 22 0.8 BRCA 1/2 positive 43 167 25 97 29 1.2 Kriege ( ) 2b Family history without BRCA mutation 1450 3409 46 95 7 0.4 BRCA 1/2 positive 329 725 32 95 15 0.8 Stoutjesdijk ( ) 3b All women ⁎ 179 262 42 96 33 1.9 Lehman ( ) 3b All women ⁎ 367 367 25 NR 25 0.3 Lehman ( ) 3b All women ⁎ 171 171 33 NR 12 1.2 Warner ( ) 4 All women ⁎ 196 196 43 100 75 1.5 Warner ( ) 4 BRCA 1/2 positive 236 457 36 100 89 1.8
CEBM, Center for Evidence-Based Medicine; NR, not reported; PPV, positive predictive value; Sens, sensitivity; Spec, specificity.
Get Radiology Tree app to read full this article<
Table 3
Breast Cancer Screening with Magnetic Resonance Imaging or Mammography in High-risk Women: Study Level Data
Study CEBM Level of Evidence Population Number of Women Screening Events Sens (%) Spec (%) PPV (%) Cancer Detection Rate (%) MARIBS ( ) 2b Family history without BRCA mutation 424 1300 100 78 3 0.8 BRCA 1 positive 139 352 92 72 11 3.4 BRCA 2 positive 86 244 92 78 18 4.5 Kuhl ( ) 2b Family history without BRCA mutation 486 1033 100 96 43 2.5 BRCA 1/2 positive 43 167 100 94 47 4.8 Kriege ( ) 2b Family history without BRCA mutation 1450 3407 92 85 4.5 0.7 BRCA 1/2 positive 329 725 84 88 16 2.2 Warner ( ) 4 All women ⁎ 196 196 100 NR NR 3.6 Warner ( ) 4 BRCA 1/2 positive 236 457 86 NR NR 4.2
CEBM, Center for Evidence-Based Medicine; NR, not reported; PPV, positive predictive value; Sens, sensitivity; Spec, specificity.
Get Radiology Tree app to read full this article<
Table 4
Summary Performances Across All Studies in All Women at Increased Risk for Breast Cancer
Imaging Modality Cancer Detection Rates (95% CI) Sensitivities (95% CI) False Positive Rates (95% CI) MRI alone 0.020 (0.011–0.028) 0.966 (0.946–0.986) 0.095 (0.037–0.153) Mammography alone 0.007 (0.004–0.009) 0.375 (0.298–0.45) 0.041 (0.024–0.057) Combination of MRI and mammography 0.019 (0.010–0.029) 0.944 (0.896–0.992) 0.138 (0.039–0.237)
CI, confidence interval; MRI, magnetic resonance imaging.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 5
Definition of a Positive Examination (by magnetic resonance imaging and mammography)
BI-RADS 0 or 3–5 BI-RADS 4–5 MARIBS ( ) Warner 2001 ( ) Stoutjesdijk ( ) Warner 2004 ( ) Kriege 2004 ( ) Kuhl ( ) Kriege 2006 ( ) Lehman 2005 ( ) Lehman 2007 ( )
BI-RADS, Breast Imaging Reporting and Data System..
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Saslow D., Boetes C., Burke W., et. al.: American Cancer Society Guidelines for breast screening with mri as an adjunct to mammography. CA Cancer J Clin 2007; 57: pp. 75-89.
2. Sheehan J.J., Ridge C.A., Ward E.V., et. al.: The process of evidence-based practice in radiology: an introduction. Acad Radiol 2007; 14: pp. 385-388.
3. Leach M.O., Boggis C.R., Dixon A.K., et. al.: Screening with magnetic resonance imaging and mammography of a UK population at high familial risk of breast cancer: a prospective multicentre cohort study (MARIBS). Lancet 2005; 365: pp. 1769-1778.
4. Kuhl C.K., Schrading S., Leutner C.C., et. al.: Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J Clin Oncol 2005; 23: pp. 8469-8476.
5. Kriege M., Brekelmans C.T.M., Obdeijn I.M., et. al.: Factors affecting sensitivity and specificity of screening mammography and MRI in women with an inherited risk for breast cancer. Breast Cancer Res Treat 2006; 100: pp. 109-119.
6. Kriege M., Brekelmans C.T.M., Boetes C., et. al.: Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med 2004; 351: pp. 427-437.
7. Stoutjesdijk M.J., Boetes C., Jager G.J., et. al.: Magnetic resonance imaging and mammography in women with a hereditary risk of breast cancer. J Natl Cancer Inst 2001; 93: pp. 1095-1102.
8. Lehman C.D., Blume J.D., Weatherall P., et. al.: Screening women at high risk for breast cancer with mammography and magnetic resonance imaging. Cancer 2005; 103: pp. 1898-1905.
9. Lehman C.D., Isaacs C., Schnall M.D., et. al.: Cancer yield of mammography, MR, and US in high-risk women: prospective multi-institution breast cancer screening study. Radiology 2007; 244: pp. 381-388.
10. Warner E., Plewes D.B., Shumak R.S., et. al.: Comparison of breast magnetic resonance imaging, mammography, and ultrasound for surveillance of women at high risk for hereditary breast cancer. J Clin Oncol 2001; 19: pp. 3524-3531.
11. Warner E., Plewes D.B., Hill K.A., et. al.: Surveillance of BRCA1 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA 2004; 292: pp. 1317-1325.
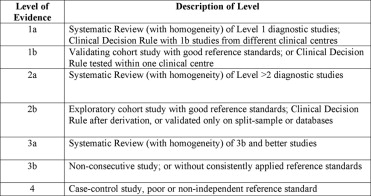
12. Centre for Evidence Based Medicine, University of Oxford: Levels of evidence and grades of recommendations. www.cebm.net/levels_of_evidence.asp Accessed August 16, 2007
13. DerSimonian R., Laird N.: Meta-analysis in clinical trials. Control Clinical Trials 1986; 7: pp. 177-188.
14. Mosteller F., Colditz G.A.: Understanding research synthesis (meta analysis). Annu Rev Public Health 1996; 17: pp. 1-23.
15. Kriege M., Brekelmans C.T., Boetes C., et. al.: Differences between first and subsequent rounds of the MRISC breast cancer screening program for women with a familial or genetic predisposition. Cancer 2006; 106: pp. 2318-2326.
16. Komenaka I.K., Ditkoff B.A., Joseph K.A., et. al.: The development of interval breast malignancies in patients with BRCA mutations. Cancer 2004; 100: pp. 2079-2083.
17. Adem C., Reynolds C., Soderberg C.L., et. al.: Pathologic characteristics of breast parenchyma in patients with hereditary breast carcinoma, including BRCA1 and BRCA2 mutation carriers. Cancer 2003; 97: pp. 1-11.