
Rationale and Objectives
Catheter ablation of the cavotricuspid isthmus (CTI) is an effective treatment of right atrial flutter. The objective of this study was to evaluate the changes in CTI length and right atrial (RA) function after radiofrequency ablation of isthmus-dependent atrial flutter (isthmus ablation).
Materials and Methods
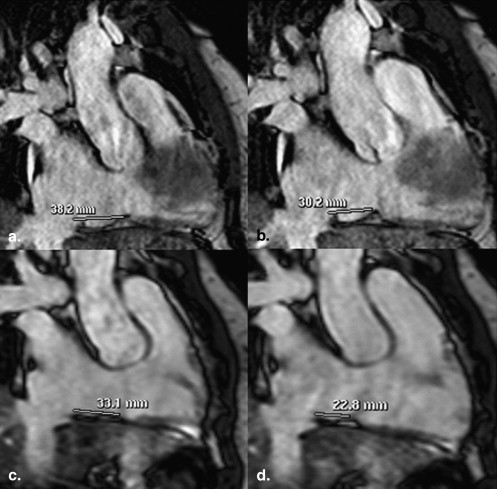
Magnetic resonance imaging was obtained in 14 patients (2 female, mean age 59 ± 9) before and after isthmus ablation (mean delay 80 ± 175 days) using steady-state free precession cine magnetic resonance imaging in right anterior oblique view orientation. Right atrial function (maximum/minimum right atrial volumes, stroke volume, ejection fraction) and maximum/minimum length of the CTI were measured.
Results
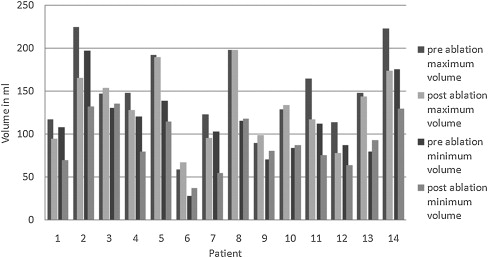
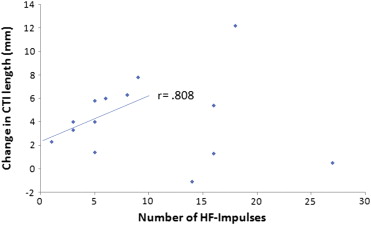
After isthmus ablation, maximum RA volume decreased by 13% ( P = .02) and minimum RA volume by 22% ( P = .01), whereas stroke volume and ejection fraction did not increase significantly ( P = .4 and .2, respectively). After ablation, the maximum length of the CTI showed a significant decrease of 19% ( P < .001) and the minimum length a decrease of 24% ( P < .001). A linear correlation between change in CTI length and number of energy applications during ablation could not be observed ( r = .605, P = .22 for minimum length; r = .384, P = .18 for maximum length). After eliminating the outliers in the number of energy applications, a significant correlation between energy applications and change in CTI systolic length was found ( r = .808, P = .008).
Conclusion
Magnetic resonance imaging to visualize right atrial size and function in right anterior oblique orientation was successfully performed and easy to evaluate for volumetric analysis and determination of CTI length. Scarring of the CTI with the use of catheter ablation leads to a significant and linear decrease in its length and to a subsequent reduction of right atrial volumes, whereas functional parameters such as stroke volume/ejection fraction did not change significantly.
Catheter ablation of the cavo-tricuspid isthmus (CTI) is an effective treatment of typical atrial flutter. The ablation aims to set a linear scar in the myocardium of the cavo-tricuspid isthmus to cut off macro-reentry mechanisms around the tricuspid valve . Although a single catheter ablation of the CTI cures about 90% of the patients with isthmus-dependent atrial flutter, reablation has to be performed in cases of recurrence and is usually successful . Anatomical characteristics can impair the ablation procedure , leading to longer ablation times and in theory to more extensive scarring of CTI . Several studies defining the right atrial isthmus either with echocardiographic or magnetic resonance imaging (MRI) have been published in the last decade, trying to address these anatomical difficulties .
In parallel to trials involving the imaging and detection of scars of the pulmonary veins after ablation, recent studies on the right atrium have analyzed changes of tissue in the ablation area of the cavo-tricuspid isthmus using MRI . Yokokawa et al studied the CTI morphology, looking at the anatomical variation of the isthmus and the prevalence of ablation-mediated tissue edema and scar formation. A postprocedural high T2-signal change and increase of wall thickness was noticed after 1 day, which resolved over the following month. The length of CTI was measured preprocedural but not after.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Atrial Flutter RFA Technique
Get Radiology Tree app to read full this article<
MRI of the Cavo-tricuspid Isthmus
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Data and Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Right Atrial Measurements Before and After Ablation
Right Atrial Measurements Preablation Postablation_P_ Value Maximum volume (mL) 148 ± 49 131 ± 42 .02 Minimum volume (mL) 111 ± 43 91 ± 31 .01 Stroke volume (mL) 38 ± 21 40 ± 20 .4 Ejection fraction (%) 26 ± 14 31 ± 10 .2 Maximum isthmus length (mm) 35 ± 8 29 ± 9 <.0001 Minimum isthmus length (mm) 22 ± 7 18 ± 6 <.001
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Cauchemez B., Haissaguerre M., Fischer B., et. al.: Electrophysiological effects of catheter ablation of inferior vena cava-tricuspid annulus isthmus in common atrial flutter. Circulation 1996; 93: pp. 284-294.
2. Feld G.K., Fleck R.P., Chen P.S., et. al.: Radiofrequency catheter ablation for the treatment of human type 1 atrial flutter. Identification of a critical zone in the reentrant circuit by endocardial mapping techniques. Circulation 1992; 86: pp. 1233-1240.
3. Saoudi N., Atallah G., Kirkorian G., et. al.: Catheter ablation of the atrial myocardium in human type I atrial flutter. Circulation 1990; 81: pp. 762-771.
4. Feld G.K., Daubert J.P., Weiss R., et. al.: Acute and long-term efficacy and safety of catheter cryoablation of the cavotricuspid isthmus for treatment of type 1 atrial flutter. Heart Rhythm 2008; 5: pp. 1009-1014.
5. Natale A., Newby K.H., Pisano E., et. al.: Prospective randomized comparison of antiarrhythmic therapy versus first-line radiofrequency ablation in patients with atrial flutter. J Am Coll Cardiol 2000; 35: pp. 1898-1904.
6. Cabrera J.A., Sanchez-Quintana D., Ho S.Y., et. al.: Angiographic anatomy of the inferior right atrial isthmus in patients with and without history of common atrial flutter. Circulation 1999; 99: pp. 3017-3023.
7. Heidbuchel H., Willems R., van Rensburg H., et. al.: Right atrial angiographic evaluation of the posterior isthmus: relevance for ablation of typical atrial flutter. Circulation 2000; 101: pp. 2178-2184.
8. Morton J.B., Sanders P., Davidson N.C., et. al.: Phased-array intracardiac echocardiography for defining cavotricuspid isthmus anatomy during radiofrequency ablation of typical atrial flutter. J Cardiovasc Electrophysiol 2003; 14: pp. 591-597.
9. Chalvidan T., Heno P., Cellarier G., et. al.: Cavo-tricuspid isthmus width in relation to the radiofrequency ablation of the common atrial flutter. Pacing Clin Electrophysiol 1999; 22: pp. 576.
10. Da Costa A., Faure E., Thevenin J., et. al.: Effect of isthmus anatomy and ablation catheter on radiofrequency catheter ablation of the cavotricuspid isthmus. Circulation 2004; 110: pp. 1030-1035.
11. Cabrera J.A., Sanchez-Quintana D., Ho S.Y., et. al.: The architecture of the atrial musculature between the orifice of the inferior caval vein and the tricuspid valve: the anatomy of the isthmus. J Cardiovasc Electrophysiol 1998; 9: pp. 1186-1195.
12. Kirchhof P., Ozgun M., Zellerhoff S., et. al.: Diastolic isthmus length and ‘vertical’ isthmus angulation identify patients with difficult catheter ablation of typical atrial flutter: a pre-procedural MRI study. Europace 2009; 11: pp. 42-47.
13. Lim K.T., Murray C., Liu H., et. al.: Pre-ablation magnetic resonance imaging of the cavotricuspid isthmus. Europace 2007; 9: pp. 149-153.
14. Okishige K., Kawabata M., Yamashiro K., et. al.: Clinical study regarding the anatomical structures of the right atrial isthmus using intra-cardiac echocardiography: implication for catheter ablation of common atrial flutter. J Interv Card Electrophysiol 2005; 12: pp. 9-12.
15. Okumura Y., Watanabe I., Ashino S., et. al.: Anatomical characteristics of the cavotricuspid isthmus in patients with and without typical atrial flutter: analysis with two- and three-dimensional intracardiac echocardiography. J Interv Card Electrophysiol 2006; 17: pp. 11-19.
16. Schwartzman D., Ren J.F., Devine W.A., et. al.: Cardiac swelling associated with linear radiofrequency ablation in the atrium. J Interv Card Electrophysiol 2001; 5: pp. 159-166.
17. Yokokawa M., Tada H., Koyama K., et. al.: The change in the tissue characterization detected by magnetic resonance imaging after radiofrequency ablation of isthmus-dependent atrial flutter. Int J Cardiol 2009 Nov 8; [Epub ahead of print]
18. Wylie J.V., Peters D.C., Essebag V., et. al.: Left atrial function and scar after catheter ablation of atrial fibrillation. Heart Rhythm 2008; 5: pp. 656-662.
19. Greenberg S.B.: Assessment of cardiac function: magnetic resonance and computed tomography. J Thorac Imaging 2000; 15: pp. 243-251.
20. Pujadas S., Reddy G.P., Weber O., et. al.: MR imaging assessment of cardiac function. J Magn Reson Imaging 2004; 19: pp. 789-799.
21. Bland J.M., Altman D.G.: Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: pp. 307-310.
22. Mahnken A.H., Gunther R.W., Krombach G.A.: [The basics of left ventricular functional analysis with MRI and MSCT]. Rofo 2004; 176: pp. 1365-1379.
23. Sievers B., Brandts B., Franken U., et. al.: Single and biplane TrueFISP cardiovascular magnetic resonance for rapid evaluation of left ventricular volumes and ejection fraction. J Cardiovasc Magn Reson 2004; 6: pp. 593-600.
24. Hergan K., Schuster A., Fruhwald J., et. al.: Comparison of left and right ventricular volume measurement using the Simpson’s method and the area length method. Eur J Radiol 2008; 65: pp. 270-278.
25. Sievers B., Addo M., Breuckmann F., et. al.: Reference right atrial function determined by steady-state free precession cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2007; 9: pp. 807-814.
26. Peters D.C., Wylie J.V., Hauser T.H., et. al.: Detection of pulmonary vein and left atrial scar after catheter ablation with three-dimensional navigator-gated delayed enhancement MR imaging: initial experience. Radiology 2007; 243: pp. 690-695.