
Rationale and Objectives
The purpose of our study was to evaluate the multidetector computed tomography (MDCT) features of benign adnexal lesions.
Methods and Materials
We report the MDCT features of 68 histologically proven benign adnexal lesions. Pathologic diagnoses were nonneoplastic adnexal cysts ( n = 16), endometriomas ( n = 12), serous or mucinous cystadenomas ( n = 15), fibromas or fibrothecomas ( n = 7), teratomas ( n = 6), and a variety of benign adnexal lesions ( n = 12). The CT protocol included scanning of the abdomen after the intravenous administration of iodinated contrast material (portal phase) using a detector collimation of 16 × 0.75 mm and a pitch of 1.2.
Results
Ovarian cysts had a characteristic CT appearance of a cystic lesion, with smooth, thin wall, and occasionally a few septa. Serous and mucinous cystadenomas were detected as multilocular cystic tumors containing serous fluid or liquids of higher than water CT density, respectively. Dilated fallopian tube was seen as an oblong, tubular, fluid-filled structure. MDCT was accurate to characterize mature cystic teratomas. Endometriomas had a variable CT appearance, including a unilocular or multilocular cystic mass, and a homogeneous hyperdense mass lesion. Fibrous tissue had a 50 HU CT density in patients with fibromas or fibrothecomas.
Conclusion
MDCT may provide accurate diagnostic information about the benign nature of adnexal lesions.
Ultrasonography remains the primary imaging modality in the workup of patients with suspected adnexal masses, with magnetic resonance imaging (MRI), although more specific in the characterization and differentiation of ovarian masses, reserved for problem-solving cases . The relatively uncommon use of computed tomography (CT) in the evaluation of benign adnexal mass lesions has resulted in a paucity of the English-language literature regarding their CT findings . Benign adnexal masses were evaluated by CT either during the investigation of an undiagnosed abdominal mass or as an incidental finding during CT examination performed for other reasons .
Multidetector CT (MDCT) greatly improved the accuracy of CT in detecting and characterizing adnexal mass lesions . Although MDCT is not considered the study of choice in the initial evaluation of adnexal masses, it proved accurate in the detection of ovarian masses, providing an accurate assessment of their internal architecture characteristics, a reliable differentiation of benign from malignant adnexal mass lesions, and an accurate preoperative staging of the disease in cases of ovarian malignancies .
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
CT Protocol
Get Radiology Tree app to read full this article<
CT Data Interpretation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
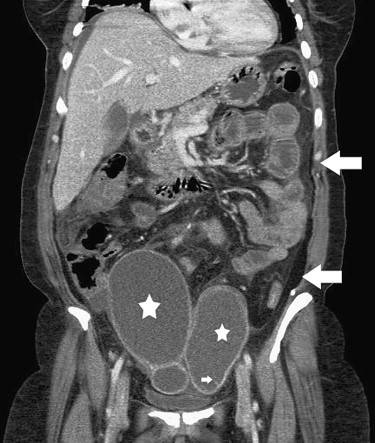
![Figure 4, Mucinous cystadenoma of the right ovary in a 40-year-old woman. (a) Coronal and (b) sagittal multiplanar reformatted images depict a huge, multicystic mass, occupying most of the abdomen. The tumor had a thin wall and innumerable, thin septa containing cystic parts (computed tomography [CT] density: 10 HU), but mainly hyperdense components (CT density: 47 HU, asterisk ). Sagittal reformation shows the presence of small papillary projections (arrows) within the lesion.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/MultidetectorCTFeaturesofBenignAdnexalLesions/3_1s20S107663320900395X.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kinkel K., Hricak H., Lu Y., et. al.: US characterization of ovarian masses: a meta-analysis. Radiology 2000; 217: pp. 803-811.
2. Hamm B., Huch-Kubic R.A., Fleige B.: MR imaging and CT of the female pelvis: radiologic-pathologic correlation. Eur Radiol 1999; 9: pp. 3-15.
3. Bazot M., Nassar-Slaba J., Thomassin-Naggara I., et. al.: MR imaging compared with intraoperative frozen-section examination for the diagnosis of adnexal tumors; correlation with final histology. Eur Radiol 2006; 16: pp. 2687-2699.
4. Sohaib S.A., Mills T.D., Sahdev A., et. al.: The role of magnetic resonance imaging and ultrasound in patients with adnexal masses. Clin Radiol 2005; 60: pp. 340-348.
5. Hricak H., Chen M., Coakley F.V., et. al.: Complex adnexal masses: detection and characterization with MR imaging-multivariate analysis. Radiology 2000; 214: pp. 39-46.
6. Sawyer R.W., Vick C.W., Walsh J.W., et. al.: Computed tomography of benign ovarian masses. J Comput Assist Tomogr 1985; 9: pp. 784-789.
7. Fukuda T., Ikeuchi M., Hashimoto H., et. al.: Computed tomography of ovarian masses. J Comput Assist Tomogr 1986; 10: pp. 990-996.
8. Fishman E.K., Scatarige J.C., Saksouk F.A., et. al.: Computed tomography of endometriosis. J Comput Assist Tomogr 1983; 7: pp. 257-264.
9. Buy J.N., Ghossain M.A., Mark A.S., et. al.: Focal hyperdense areas in endometriomas: a characteristic finding on CT. AJR Am J Roentgenol 1992; 159: pp. 769-771.
10. Bazot M., Ghossain M.A., Buy J.N., et. al.: Fibrothecomas of the ovary: CT and US findings. J Comput Assist Tomogr 1993; 17: pp. 754-759.
11. Tsili A.C., Tsampoulas C., Argyropoulou M., et. al.: Comparative evaluation of multidetector CT and MR imaging in the differentiation of adnexal masses. Eur Radiol 2008; 18: pp. 1049-1057.
12. Tsili A.C., Tsampoulas C., Charisiadi A., et. al.: Adnexal masses: accuracy of detection and differentiation with multidetector computed tomography. Gynecol Oncol 2008; 110: pp. 22-31.
13. Forstner R.: Radiological staging of ovarian cancer: imaging findings and contribution of CT and MRI. Eur Radiol 2007; 17: pp. 3223-3235.
14. Karla M.K., Maher M.M., Toth T.L., et. al.: Techniques and applications of automatic tube current modulation for CT. Radiology 2004; 233: pp. 649-657.
15. Rha S.E., Byun J.Y., Jung S.E., et. al.: CT and MR imaging features of adnexal torsion. Radiographics 2002; 22: pp. 283-294.
16. Jung S.E., Lee J.M., Rha S.E., et. al.: CT and MR imaging of ovarian tumors with emphasis on differential diagnosis. Radiographics 2002; 22: pp. 1305-1325.
17. Kawamoto S., Urban B.A., Fishman E.K.: CT of epithelial ovarian tumors. Radiographics 1999; 19: pp. S85-S102.
18. Outwater E.K., Huang A.B., Dunton C.J., et. al.: Papillary projections in ovarian neoplasms: appearance on MRI. J Magn Reson Imaging 1997; 7: pp. 689-695.
19. Outwater E.K., Wagner B.J., Mannion C., et. al.: From the archives of the AFIP. Sex cord-stromal and steroid cell tumors of the ovary. Radiographics 1998; 18: pp. 1523-1546.
20. Outwater E.K., Siegelman E.S., Hunt J.L.: Ovarian teratomas: tumor types and imaging characteristics. Radiographics 2001; 21: pp. 475-490.
21. Guinet C., Ghossain M.A., Buy J.N., et. al.: Mature cystic teratomas of the ovary: CT and MR findings. Eur J Radiol 1995; 20: pp. 137-143.
22. Tsushima Y., Kita T., Yamamoto K.: Uterine lipoleiomyoma: MRI, CT and ultrasonographic findings. Br J Radiol 1997; 70: pp. 1068-1070.
23. Sam J.W., Jacobs J.E., Birnbaum B.A.: Spectrum of CT findings in acute pyogenic pelvic inflammatory disease. Radiographics 2002; 22: pp. 1327-1334.
24. Outwater E.K., Siegelman E.S., Chiowanich P., et. al.: Dilated fallopian tubes: MR imaging characteristics. Radiology 1998; 208: pp. 463-469.
25. Susumu O., Yoshiharu O., Takashi K., et. al.: Cystic struma ovarii: Imaging findings. J Comput Assist Tomogr 2000; 24: pp. 413-415.
26. Matsuki M., Kaji Y., Matsuo M., et. al.: Struma ovarii: MRI findings. Br J Radiol 2000; 73: pp. 87-90.