
Rationale and Objectives
The aim of this prospective study was to investigate using multiparametric and multinuclear magnetic resonance imaging during preoperative systemic therapy for locally advanced breast cancer.
Materials and Methods
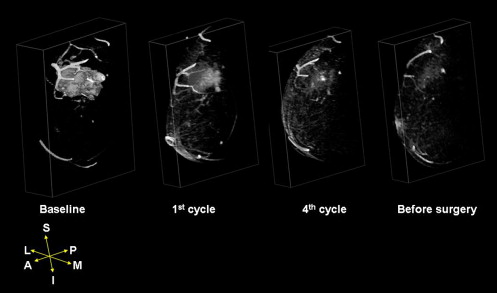
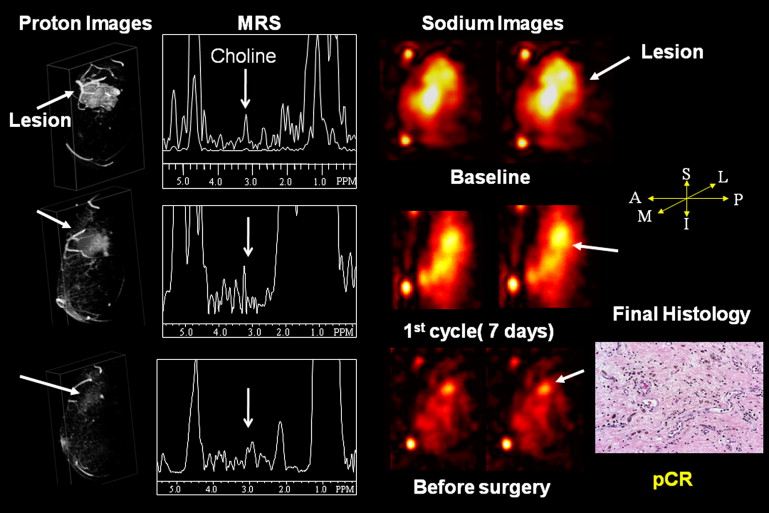
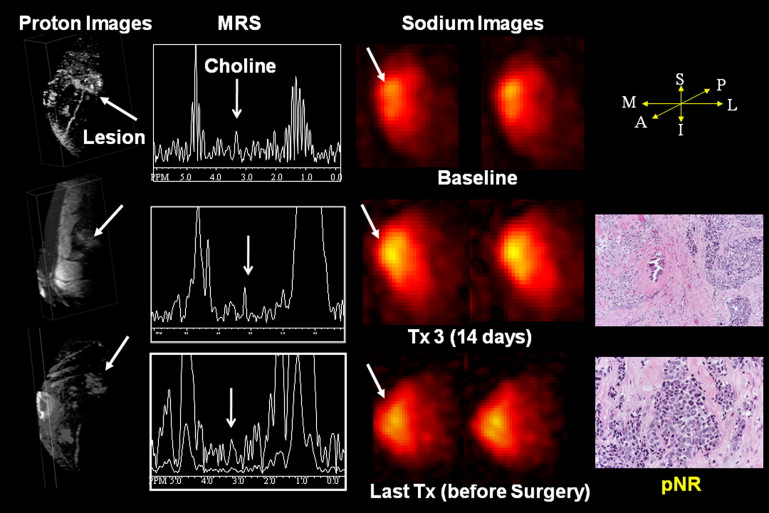
Women with operable stage 2 or 3 breast cancer who received preoperative systemic therapy were studied using dynamic contrast-enhanced magnetic resonance imaging, magnetic resonance spectroscopy, and 23 Na magnetic resonance. Quantitative metrics of choline peak signal-to-noise ratio, total tissue sodium concentration, tumor volumes, and Response Evaluation Criteria in Solid Tumors were determined and compared to final pathologic results using receiver-operating characteristic analysis. Hormonal markers were investigated. Statistical significance was set at P < .05.
Results
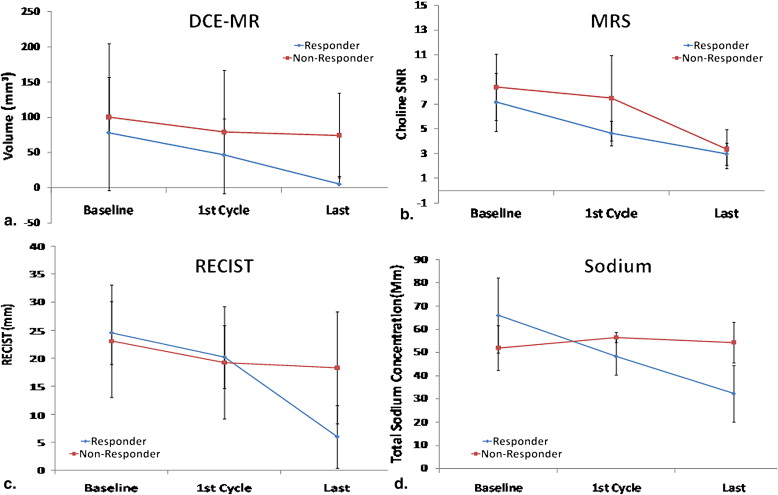
Eighteen eligible women were studied. Fifteen responded to therapy, four (22%) with pathologic complete response and 11 (61%) with pathologic partial response. Three patients (17%) had no response. Among estrogen receptor–positive, HER2-positive, and triple-negative phenotypes, observed frequencies of pathologic complete response, pathologic partial response, and no response were 2, 5, and 0; 1, 4, and 0; and 1, 1, and 3, respectively. Responders (pathologic complete response and pathologic partial response) had the largest reductions in choline signal-to-noise ratio (35%, from 7.2 ± 2.3 to 4.6 ± 2; P < .01) compared to nonresponders (11%, from 8.4 ± 2.7 to 7.5 ± 3.6; P = .13) after the first cycle. Total tissue sodium concentration significantly decreased in responders (27%, from 66 ± 18 to 48.4 ± 8 mmol/L; P = .01), while there was little change in nonresponders (51.7 ± 7.6 to 56.5 ± 1.6 mmol/L; P = .50). Lesion volume decreased in responders (40%, from 78 ± 78 to 46 ± 51 mm 3 ; P = .01) and nonresponders (21%, from 100 ± 104 to 79.2 ± 87 mm 3 ; P = .23) after the first cycle. The largest reduction in Response Evaluation Criteria in Solid Tumors occurred after the first treatment in responders (18%, from 24.5 ± 20 to 20.2 ± 18 mm; P = .01), with a slight decrease in tumor diameter noted in nonresponders (17%, from 23 ± 19 to 19.2 ± 19.1 mm; P = .80).
Conclusions
Multiparametric and multinuclear imaging parameters were significantly reduced after the first cycle of preoperative systemic therapy in responders, specifically, choline signal-to-noise ratio and sodium. These new surrogate radiologic biomarkers maybe able to predict and provide a platform for potential adaptive therapy in patients.
Breast cancer is a potentially curable disease, and the combined effects of early detection and adjuvant systemic therapy are likely the key elements that explain the observed reduction in breast cancer mortality over the past 20 years . The currently accepted standards for the detection and diagnosis of breast abnormalities are mammography, ultrasound, and magnetic resonance (MR) imaging (MRI) . If breast lesions are detected early, adjuvant systemic therapy after primary surgery reduces the risk for systemic recurrence or death . However, not all breast cancers are detected early, and some patients may present with stage 2 or 3 disease and require multimodality therapy. Preoperative systemic therapy (PST), also referred to as primary or neoadjuvant chemotherapy, is used to potentially reduce the size of the tumor and possibly convert a mastectomy to a lumpectomy in primary operable or locally advanced breast cancer . Perhaps of greater therapeutic implications, it may allow an early assessment of disease responsiveness and an opportunity to adjust therapy on the basis of observed response .
Pathologic response following PST appears to correlate with long-term outcome. National Surgical Adjuvant Bowel and Breast Project trial protocol B18 showed that approximately 12% of patients had pathologic complete response (pCR) with an anthracycline-based regimen (eg, doxorubicin and cyclophosphamide [AC]) , while the addition of four more cycles of a taxane in National Surgical Adjuvant Bowel and Breast Project trial protocol B27 doubled the pCR rate compared to AC alone . Patients who achieved pCR in these two studies had longer disease-free and overall survival . If this is confirmed, it implies that the early identification of those likely to respond to PST is of critical importance as a prognostic marker and to potentially allow midcourse adjustments in therapy. Thus, in vivo assessment before, during, and after PST may improve decision making and outcomes. Recent studies have demonstrated that in vivo assessments of therapeutic response are possible using MRI in patients who are undergoing PST . Partridge et al demonstrated that the use of dynamic contrast-enhanced (DCE) MRI could be predictive of outcome after a reduction in the size of the tumor in a recent American College of Radiology Imaging Network multi-institutional center trial. Messiamy et al reported that the use of MR spectroscopy (MRS) within 24 to 48 hours after the first cycle of therapy could detect cellular changes in total choline concentration within the tumor, and this has been confirmed by others . In addition, recent reports have demonstrated that the use of 23 Na MRI in patients with breast and other diseases provides additional metabolic information for diagnosis .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Clinical Subjects
Get Radiology Tree app to read full this article<
Pathologic Response and Histologic Tissue Classification
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MRI Protocol
Proton MRI
Get Radiology Tree app to read full this article<
Proton MRS
Get Radiology Tree app to read full this article<
23 Na MRI
Get Radiology Tree app to read full this article<
MR Image Preprocessing and Analysis
Lesion and Volume Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MR Spectroscopic Analysis
Get Radiology Tree app to read full this article<
Quantitative 23 Na MRI
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Clinical and Histopathologic Characteristics
Get Radiology Tree app to read full this article<
Table 1
Patient Characteristics and Treatment Response ( n = 18)

AUC, area under the receiver-operating characteristic curve; DCE, dynamic contrast-enhanced; ER, estrogen receptor; FISH, fluorescence in situ hybridization; IHC, immunohistochemistry; PR, progesterone receptor; RECIST, Response Evaluation Criteria in Solid Tumors.
Get Radiology Tree app to read full this article<
Clinical Response and Pathology Findings After PST
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiologic Metrics
General
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
RECIST
Get Radiology Tree app to read full this article<
MRS
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
23 Na MRI
Get Radiology Tree app to read full this article<
Proton DCE MR
Get Radiology Tree app to read full this article<
Subgroup Analysis Between Pathologic Response, Tumor Phenotype, and Imaging Findings
TN Phenotype
Get Radiology Tree app to read full this article<
ER-negative, Progesterone Receptor (PR)–negative, and HER2-positive Phenotype
Get Radiology Tree app to read full this article<
ER-positive, PR-positive, and HER2-negative Phenotype
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Jemal A., Siegel R., Ward E., et. al.: Cancer statistics, 2009. CA Cancer J Clin 2009; 59: pp. 225-249.
2. Lehman C.D., Gatsonis C., Kuhl C.K., et. al.: MRI evaluation of the contralateral breast in women with recently diagnosed breast cancer. N Engl J Med 2007; 356: pp. 1295-1303.
3. El Khouli R.H., Jacobs M.A., Bluemke D.A.: Magnetic resonance imaging of the breast. Semin Roentgenol 2008; 43: pp. 265-281.
4. Early Breast Cancer Trialists’ Collaborative Group: Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005; 365: pp. 1687-1717.
5. Wolff A.C., Berry D., Carey L.A., et. al.: Research issues affecting preoperative systemic therapy for operable breast cancer. J Clin Oncol 2008; 26: pp. 806-813.
6. Fisher B., Redmond C., Brown A., et. al.: Adjuvant chemotherapy with and without tamoxifen in the treatment of primary breast cancer: 5-year results from the National Surgical Adjuvant Breast and Bowel Project Trial. J Clin Oncol 1986; 4: pp. 459-471.
7. Fisher B., Redmond C., Wickerham D.L., et. al.: Systemic therapy in patients with node-negative breast cancer. A commentary based on two National Surgical Adjuvant Breast and Bowel Project (NSABP) clinical trials. Ann Intern Med 1989; 111: pp. 703-712.
8. Kaufmann M., Hortobagyi G.N., Goldhirsch A., et. al.: Recommendations from an international expert panel on the use of neoadjuvant (primary) systemic treatment of operable breast cancer: an update. J Clin Oncol 2006; 24: pp. 1940-1949.
9. Fisher B., Bryant J., Wolmark N., et. al.: Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J Clin Oncol 1998; 16: pp. 2672-2685.
10. National Surgical Adjuvant Breast and Bowel Project: The effect on primary tumor response of adding sequential Taxotere to Adriamycin and cyclophosphamide: preliminary results from NSABP protocol B-27. Breast Cancer Res Treat 2001; 69: pp. 215.
11. Esserman L., Hylton N., Yassa L., et. al.: Utility of magnetic resonance imaging in the management of breast cancer: evidence for improved preoperative staging. J Clin Oncol 1999; 17: pp. 110-119.
12. Partridge S.C., Gibbs J.E., Lu Y., et. al.: MRI measurements of breast tumor volume predict response to neoadjuvant chemotherapy and recurrence-free survival. AJR Am J Roentgenol 2005; 184: pp. 1774-1781.
13. Yu H.J., Chen J.H., Mehta R.S., et. al.: MRI measurements of tumor size and pharmacokinetic parameters as early predictors of response in breast cancer patients undergoing neoadjuvant anthracycline chemotherapy. J Magn Reson Imaging 2007; 26: pp. 615-623.
14. Meisamy S., Bolan P.J., Baker E.H., et. al.: Neoadjuvant chemotherapy of locally advanced breast cancer: predicting response with in vivo 1H MR spectroscopy—a pilot study at 4 T. Radiology 2004; 233: pp. 424-431.
15. Manton D.J., Chaturvedi A., Hubbard A., et. al.: Neoadjuvant chemotherapy in breast cancer: early response prediction with quantitative MR imaging and spectroscopy. Br J Cancer 2006; 94: pp. 427-435.
16. Kumar V., Jagannathan N.R., Kumar R., et. al.: Correlation between metabolite ratios and ADC values of prostate in men with increased PSA level. Magn Reson Imaging 2006; 24: pp. 541-548.
17. Baek H.M., Chen J.H., Nie K., et. al.: Predicting pathologic response to neoadjuvant chemotherapy in breast cancer by using MR imaging and quantitative 1H MR spectroscopy. Radiology 2009; 251: pp. 653-662.
18. Jacobs M.A., Ouwerkerk R., Wolff A.C., et. al.: Multiparametric and multinuclear magnetic resonance imaging of human breast cancer: current applications. Technol Cancer Res Treat 2004; 3: pp. 543-550.
19. Ouwerkerk R., Jacobs M.A., Macura K.J., et. al.: Elevated tissue sodium concentration in malignant breast lesions detected with non-invasive (23)Na MRI. Breast Cancer Res Treat 2007; 106: pp. 151-160.
20. Jacobs M.A., Ouwerkerk R., Kamel I., et. al.: Proton, diffusion-weighted imaging, and sodium ((23)Na) MRI of uterine leiomyomata after MR-guided high-intensity focused ultrasound: a preliminary study. J Magn Reson Imaging 2009; 29: pp. 649-656.
21. Bottomley P.A.: Spatial localization in NMR spectroscopy in vivo. Ann N Y Acad Sci 1987; 508: pp. 333-348.
22. Jacobs M.A., Barker P.B., Bluemke D.A., et. al.: Benign and malignant breast lesions: diagnosis with multiparametric MR imaging. Radiology 2003; 229: pp. 225-232.
23. Haase A., Frahm J., Hanicke W., et. al.: H-1-NMR chemical-shift selective (CHESS) imaging. Phys Med Biol 1985; 30: pp. 341-344.
24. Therasse P., Eisenhauer E.A., Verweij J.: RECIST revisited: a review of validation studies on tumour assessment. Eur J Cancer 2006; 42: pp. 1031-1039.
25. Eisenhauer E.A., Therasse P., Bogaerts J., et. al.: New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009; 45: pp. 228.
26. Jacobs M.A., Knight R.A., Windham J.P., et. al.: Identification of cerebral ischemic lesions in rat using eigenimage filtered magnetic resonance imaging. Brain Res 1999; 837: pp. 83-94.
27. Jacobs M.A., Barker P.B., Bottomley P.A., et. al.: Proton MR spectroscopic imaging of human breast cancer: a preliminary study. J Magn Reson Imaging 2004; 19: pp. 68-75.
28. Baek H.M., Yu H.J., Chen J.H., et. al.: Quantitative correlation between (1)H MRS and dynamic contrast-enhanced MRI of human breast cancer. Magn Reson Imaging 2008; 26: pp. 523-531.
29. Ouwerkerk R., Bleich K.B., Gillen J.S., et. al.: Tissue sodium concentration in human brain tumors as measured with 23Na MR imaging. Radiology 2003; 227: pp. 529-537.
30. Ouwerkerk R., Weiss R.G., Bottomley P.A.: Measuring human cardiac tissue sodium concentrations using surface coils, adiabatic excitation, and twisted projection imaging with minimal T2 losses. J Magn Reson Imaging 2005; 21: pp. 546-555.
31. Hilal S.K., Maudsley A.A., Ra J.B., et. al.: In vivo NMR imaging of sodium-23 in the human head. J Comput Assist Tomogr 1985; 9: pp. 1-7.
32. Nagy I., Lustyik G., Lukacs G., et. al.: Correlation of malignancy with the intracellular Na+:K+ ratio in human thyroid tumors. Cancer Res 1983; 43: pp. 5395-5402.
33. Navon G.: Complete elimination of the extracellular 23Na NMR signal in triple quantum filtered spectra of rat hearts in the presence of shift reagents. Magn Reson Med 1993; 30: pp. 503-506.
34. Kline R.P., Wu E.X., Petrylak D.P., et. al.: Rapid in vivo monitoring of chemotherapeutic response using weighted sodium magnetic resonance imaging. Clin Cancer Res 2000; 6: pp. 2146-2156.
35. Winter P.M., Poptani H., Bansal N.: Effects of chemotherapy by 1,3-bis(2-chloroethyl)-1-nitrosourea on single-quantum- and triple-quantum-filtered 23Na and 31P nuclear magnetic resonance of the subcutaneously implanted 9L glioma. Cancer Res 2001; 61: pp. 2002-2007.
36. Babsky A.M., Topper S., Zhang H., et. al.: Evaluation of extra- and intracellular apparent diffusion coefficient of sodium in rat skeletal muscle: effects of prolonged ischemia. Magn Reson Med 2008; 59: pp. 485-491.
37. Pike M.M., Frazer J.C., Dedrick D.F., et. al.: 23Na and 39K nuclear magnetic resonance studies of perfused rat hearts. Discrimination of intra- and extracellular ions using a shift reagent. Biophys J 1985; 48: pp. 159-173.
38. Pekar J., Renshaw P.F., Leigh J.S.: Selective detection of intracellular sodium by coherence-transfer NMR. J Magn Reson 1987; 72: pp. 159-161.
39. Winter P.M., Bansal N.: Triple-quantum-filtered 23Na NMR spectroscopy of subcutaneously implanted 9L gliosarcoma in the rat in the presence of TmDOTP5-. J Magn Reson 2001; 152: pp. 70-78.
40. Tanase C., Boada F.E.: Triple-quantum-filtered imaging of sodium in presence of B(0) inhomogeneities. J Magn Reson 2005; 174: pp. 270-278.
41. Glunde K., Jacobs M.A., Pathak A.P., et. al.: Molecular and functional imaging of breast cancer. NMR Biomed 2009; 22: pp. 92-103.
42. Glunde K., Jacobs M.A., Bhujwalla Z.M.: Choline metabolism in cancer: implications for diagnosis and therapy. Expert Rev Mol Diagn 2006; 6: pp. 821-829.
43. Negendank W., Li C.W., Padavic-Shaller K., et. al.: Phospholipid metabolites in 1H-decoupled 31P MRS in vivo in human cancer: implications for experimental models and clinical studies. Anticancer Res 1996; 16: pp. 1539-1544.
44. Soher B.J., van Zijl P.C., Duyn J.H., et. al.: Quantitative proton MR spectroscopic imaging of the human brain. Magn Reson Med 1996; 35: pp. 356-363.
45. Bolan P.J., Meisamy S., Baker E.H., et. al.: In vivo quantification of choline compounds in the breast with 1H MR spectroscopy. Magn Reson Med 2003; 50: pp. 1134-1143.
46. Baik H.M., Su M.Y., Yu H., et. al.: Quantification of choline-containing compounds in malignant breast tumors by 1H MR spectroscopy using water as an internal reference at 1.5 T. Magma 2006; 19: pp. 96-104.
47. Fayad L.M., Salibi N., Wang X., et. al.: Quantification of muscle choline concentrations by proton MR spectroscopy at 3 T: technical feasibility. AJR Am J Roentgenol 2010; 194: pp. W73-W79.
48. Woodhams R., Matsunaga K., Iwabuchi K., et. al.: Diffusion-weighted imaging of malignant breast tumors: the usefulness of apparent diffusion coefficient (ADC) value and ADC map for the detection of malignant breast tumors and evaluation of cancer extension. J Comput Assist Tomogr 2005; 29: pp. 644-649.
49. El Khouli R.H., Macura K.J., Barker P.B., et. al.: Relationship of temporal resolution to diagnostic performance for dynamic contrast enhanced MRI of the breast. J Magn Reson Imaging 2009; 30: pp. 999-1004.
50. Jin G., An N., Jacobs M.A., Li K.: The role of parallel diffusion-weighted imaging and apparent diffusion coefficient (ADC) map values for evaluating breast lesions: preliminary results. Acad Radiol 2010; 17: pp. 456-463.
51. El Khouli R.H., Jacobs M.A., Macura K.J., et. al.: Diffusion weighted imaging improves the diagnostic accuracy of conventional breast MRI at 3 tesla. Radiology 2010; 256: pp. 64-73.