
Rationale and Objectives
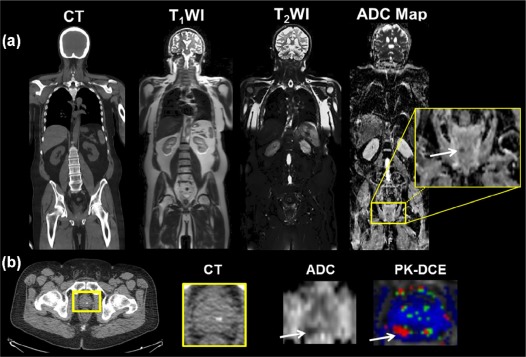
The purpose of this study was to investigate the use of multiparametric, whole-body, diffusion-weighted imaging (WB-DWI) and apparent diffusion coefficient (ADC) maps with T 2 -weighted magnetic resonance imaging (MRI) at 3T for the detection and monitoring of metastatic disease in patients.
Materials and Methods
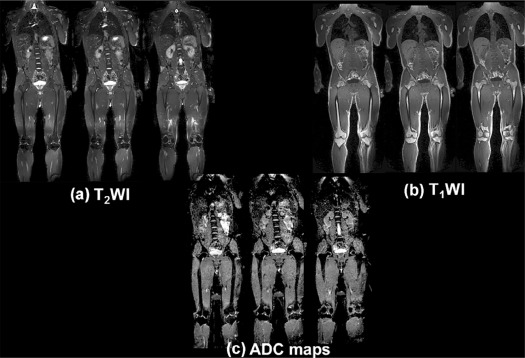
Fifty-four participants (32 healthy subjects and 22 patients) were scanned with WB-DWI methods using a 3T MRI scanner. Axial, sagittal, or coronal fat-suppressed T 2 -weighted (T 2 WI), T 1 -weighted (T 1 WI), and DWI images were acquired. Total MRI acquisition and set-up time was approximately 45 minutes. Metastatic disease on MRI was confirmed based on T 2 WI characteristics. The number of lesions was established on computed tomography (CT) or positron emission tomography (PET-CT). Whole-body ADC maps and T 2 WI were constructed, and region-of-interests were drawn in normal and abnormal-appearing tissue for quantitative analysis. Statistical analysis was performed using a paired t tests and P < .05 was considered statistically significant.
Results
There were 91 metastatic lesions detected from the CT or PET-CT with a missed recurrent lesion in the prostate. Multiparametric WB-MRI had excellent sensitivity (96%) for detection of metastatic lesions compared to CT. ADC map values and the ADC ratio in metastatic bone lesions were significantly increased ( P < .05) compared to normal bone. In soft tissue, ADC map values and ratios in metastatic lesions were decreased compared to normal soft tissue.
Conclusion
We have demonstrated that multiparametric WB-MRI is feasible for oncologic staging to identify bony and visceral metastasis in breast, prostate, pancreatic, and colorectal cancers. WB-MRI can be tailored to fit the patient, such that an “individualized patient sequence” can be developed for a comprehensive evaluation for staging and response during treatment.
Introduction
Metastatic disease or local recurrences of cancer have an unfavorable prognosis. Treatment approaches for distant metastases are mostly palliative rather than curative. Skeletal or organ metastasis is usually not detected until clinical symptoms appear, or during initial staging of cancer by imaging . If metastatic disease is found, most patients will receive various systemic therapy regimens, with the goal of ameliorating symptoms and improving survival. Although positron emission tomography-computed tomography (PET-CT) covers most of the body, measures the metabolic activity of a tumor, and is used for staging and treatment response, PET may be limited by other factors, such as high uptake in normal organs, variability in tracer uptake in lesions, increased radiation dose, or indeterminate findings due to the size of the lesion (less than 1 cm) . Therefore, there is a need for an imaging method that achieves global tumor assessment and accurate lesion detection for increased confidence in the detection, characterization, and monitoring of treatment response in metastatic disease without an increase in radiation dose.
To address these challenges, developments in whole-body MRI (WB-MRI) technology have resulted in whole-body coverage using anatomic T 1 - or T 2 -weighted imaging at 1.5T . Some of the improvements are specialized surface coils, continuous table movement (CTM), improved respiratory gating, planning software, and pulse sequences. These system improvements in MRI technology have led to impressive results in both oncological and nononcological applications of WB-MRI compared to more conventional imaging methods . As it turns out, most of the applications have been limited to anatomic and qualitative MRI parameters. There is a growing need to accurately quantify functional properties of the tissue, because these metrics represent early biological changes before anatomic MRI parameters. In particular, advanced quantitative MRI parameters such as diffusion-weighted imaging (DWI) with apparent diffusion coefficient (ADC) maps, and dynamic contrast-enhanced-MRI (DCE) can provide metrics of the molecular and vascular characteristics of tumors . There are several reports in the literature about the feasibility of using WB-DWI in different cancers . However, only a few of these WB-DWI methods have been applied to whole-body imaging at 3T . Therefore, we have implemented multiparametric WB-MRI, coupled with DWI and quantitative ADC mapping at 3T, to provide functional and quantitative information about normal and tumor (primary or metastatic) tissue and compare the WB-MRI results to CT or PET-CT results. This development of quantitative DWI WB-MRI provides the opportunity to investigate the detection and characterization of metastatic areas in the body without the need for ionizing radiation.
Materials and Methods
Clinical Subjects
Get Radiology Tree app to read full this article<
Metastatic Lesion Classification
Get Radiology Tree app to read full this article<
MRI Imaging
WB-MRI Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Proton MR Imaging
Get Radiology Tree app to read full this article<
Quantitative Diffusion-Weighted Imaging and Apparent Diffusion Coefficient Mapping
Get Radiology Tree app to read full this article<
2D PACE Respiratory Gating
Get Radiology Tree app to read full this article<
Computed Tomography and Positron Emission Tomography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiological Image Preprocessing and Analysis
Normal and Lesion Tissue Analysis
Get Radiology Tree app to read full this article<
NormalizedADCvalue=ADCvalueoflesionADCvalueofnormaltissue Normalized
ADC
value
=
ADC
value
of
lesion
ADC
value
of
normal
tissue
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Clinical Characteristics
Get Radiology Tree app to read full this article<
Radiological Metrics
Conventional Metastatic Imaging
Get Radiology Tree app to read full this article<
WB-MRI
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Diffusion-Weighted Imaging-ADC Mapping
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 1
Regional ADC Map Values From Healthy Subjects
Normals (n = 32) ADC 10 −3 mm 2 /s ADC 10 −3 mm 2 /s Tissue Normal (Rt) SD (±) Normal (Lt) SD (±) ADC ratio Cerebral cortex 0.83 0.14 0.83 0.06 1.00 Cerebellum 0.68 0.06 0.70 0.06 0.97 Lateral ventricle 3.01 0.41 3.14 0.19 0.96 Breast glandular 1.94 0.33 1.91 0.27 1.02 Gall bladder 2.85 0.28 Liver 1.16 0.22 1.12 0.26 1.04 Spleen 0.79 0.07 Pancreas(tail) 1.40 0.19 Kidney 1.93 0.14 1.94 0.11 0.99 Prostate (PZ) 1.68 0.17 1.69 0.23 0.99 Iliac crest 0.43 0.17 0.45 0.18 0.96 Femur 0.21 0.16 0.23 0.15 0.91 Pelvis 0.43 0.13 0.48 0.18 0.90 Psoas muscle 1.35 0.23 1.34 0.20 1.01 Urinary bladder 3.20 0.21 Uterus 1.27 0.20 Vertebral disk 1.59 0.19 Vertebral bone (cervical) 0.43 0.18 Vertebral bone (thoracic) 0.29 0.20 Vertebral bone (lumbar) 0.33 0.20
ADC, apparent diffusion coefficient; Lt, Left; PZ, peripheral zone; Rt, right; SD, standard deviation.
ADC Ratio = contralateral tissue divided by ipsilateral tissue ADC map values.
TABLE 2
Regional Normal ADC Map Values From Patients
Patients (n = 22) ADC 10 −3 mm 2 /s ADC 10 −3 mm 2 /s Tissue Normal (Rt) SD (±) Normal (Lt) SD (±) ADC ratio Cerebral cortex 0.82 0.08 0.84 0.14 0.98 Cerebellum 0.67 0.12 0.66 0.12 1.02 Lateral ventricle 3.30 0.24 3.23 0.22 1.02 Breast glandular 1.85 0.58 1.61 0.08 1.15 Gall bladder 2.75 0.20 Liver 0.99 0.24 1.01 0.22 0.98 Spleen 0.78 0.11 Pancreas(tail) 1.54 0.24 Kidney 1.85 0.17 1.85 0.13 1.00 Prostate (PZ) 1.45 0.15 1.42 0.10 1.02 Iliac crest 0.31 0.19 0.32 0.20 0.97 Femur 0.17 0.15 0.23 0.17 0.74 Pelvis 0.32 0.14 0.24 0.26 1.33 Psoas muscle 1.19 0.27 1.32 0.19 0.90 Urinary bladder 2.90 0.24 Uterus 1.42 0.13 Vertebral disk 1.53 0.16 Vertebral bone (cervical) 0.60 0.17 Vertebral bone (thoracic) 0.27 0.18 Vertebral bone (lumbar) 0.33 0.21
ADC, apparent diffusion coefficient; Lt, Left; PZ, peripheral zone; Rt, right; SD, standard deviation.
Ratio = contralateral tissue divided by ipsilateral tissue ADC map values.
TABLE 3
ADC Map Values From Metastatic Lesions in Patients
Metastatic Lesions ADC 10 −3 mm 2 /s ADC 10 − mm 2 /s Tissue Lesion SD (±) Normal SD (±) Ratio Vertebral bone (thoracic) 0.82 0.13 0.27 0.18 3.04 Vertebral bone (lumbar) 0.99 0.19 0.33 0.21 3.00 Pelvis 0.90 0.10 0.17 0.15 5.29 Femur 1.60 0.23 0.32 0.14 5.00 Iliac crest 0.84 0.45 0.32 0.07 2.63 Liver 0.88 0.27 1.12 0.26 0.79 Prostate (PZ) 1.00 0.07 1.45 0.15 0.69
ADC, apparent diffusion coefficient; Lt, left; PZ, peripheral zone; Rt, right; SD, standard deviation.
Ratio = Lesion tissue divided by normal tissue ADC.
Get Radiology Tree app to read full this article<
ADC Ratios and Standardized Uptake Values in Normal and Lesion Tissue
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Hortobagyi G.N.: Bone metastases in breast cancer patients. Semin Oncol 1991; 18: pp. 11-15.
2. Lu J., Steeg P.S., Price J.E., et. al.: Breast cancer metastasis: challenges and opportunities. Cancer Res 2009; 69: pp. 4951-4953.
3. Cook G.J., Houston S., Rubens R., et. al.: Detection of bone metastases in breast cancer by 18FDG PET: differing metabolic activity in osteoblastic and osteolytic lesions. J Clin Oncol 1998; 16: pp. 3375-3379.
4. Yang H.L., Liu T., Wang X.M., et. al.: Diagnosis of bone metastases: a meta-analysis comparing 18FDG PET, CT, MRI and bone scintigraphy. Eur Radiol 2011; 21: pp. 2604-2617.
5. Ballon D., Dyke J., Schwartz L.H., et. al.: Bone marrow segmentation in leukemia using diffusion and T (2) weighted echo planar magnetic resonance imaging. NMR Biomed 2000; 13: pp. 321-328.
6. Daldrup-Link H.E., Franzius C., Link T.M., et. al.: Whole-body MR imaging for detection of bone metastases in children and young adults: comparison with skeletal scintigraphy and FDG PET. Am J Roentgenol 2001; 177: pp. 229-236.
7. Hargaden G., O’Connell M., Kavanagh E., et. al.: Current concepts in whole-body imaging using turbo short tau inversion recovery MR imaging. Am J Roentgenol 2003; 180: pp. 247-252.
8. Johnston C., Brennan S., Ford S., et. al.: Whole body MR imaging: applications in oncology. Eur J Surg Oncol 2006; 32: pp. 239-246.
9. Li S., Sun F., Jin Z.Y., et. al.: Whole-body diffusion-weighted imaging: technical improvement and preliminary results. J Magn Reson Imaging 2007; 26: pp. 1139-1144.
10. Stecco A., Romano G., Negru M., et. al.: Whole-body diffusion-weighted magnetic resonance imaging in the staging of oncological patients: comparison with positron emission tomography computed tomography (PET-CT) in a pilot study. Radiol Med 2009; 114: pp. 1-17.
11. Karpitschka M., Godau-Kellner P., Kellner H., et. al.: Assessment of therapeutic response in ankylosing spondylitis patients undergoing anti-tumour necrosis factor therapy by whole-body magnetic resonance imaging. Eur Radiol 2013; 23: pp. 1773-1784.
12. Blackledge M.D., Collins D.J., Tunariu N., et. al.: Assessment of treatment response by total tumor volume and global apparent diffusion coefficient using diffusion-weighted MRI in patients with metastatic bone disease: a feasibility study. PLoS ONE 2014; 9: e91779; PMCID: PMC3977851
13. Chhabra A., Carrino J.A., Farahani S.J., et. al.: Whole-body MR neurography: prospective feasibility study in polyneuropathy and Charcot-Marie-Tooth disease. J Magn Reson Imaging 2016; 44: pp. 1513-1521.
14. Axelsen M.B., Eshed I., Ostergaard M., et. al.: Monitoring total-body inflammation and damage in joints and entheses: the first follow-up study of whole-body magnetic resonance imaging in rheumatoid arthritis. Scand J Rheumatol 2017; 46: pp. 253-262.
15. Chenevert T.L., Stegman L.D., Taylor J.M., et. al.: Diffusion magnetic resonance imaging: an early surrogate marker of therapeutic efficacy in brain tumors. J Natl Cancer Inst 2000; 92: pp. 2029-2036.
16. de Souza N.M., Riches S.F., Vanas N.J., et. al.: Diffusion-weighted magnetic resonance imaging: a potential non-invasive marker of tumour aggressiveness in localized prostate cancer. Clin Radiol 2008; 63: pp. 774-782.
17. Padhani A.R., Liu G., Mu-Koh D., et. al.: Diffusion-weighted magnetic resonance imaging as a cancer biomarker: consensus and recommendations. Neoplasia 2009; 11: pp. 102-125.
18. Ei Khouli R.H., Jacobs M.A., Mezban S.D., et. al.: Diffusion-weighted imaging improves the diagnostic accuracy of conventional 3.0-T breast MR imaging. Radiology 2010; 256: pp. 64-73.
19. Takahara T., Imai Y., Yamashita T., et. al.: Diffusion weighted whole body imaging with background body signal suppression (DWIBS): technical improvement using free breathing, STIR and high resolution 3D display. Radiat Med 2004; 22: pp. 275-282.
20. Koh D.M., Takahara T., Imai Y., et. al.: Practical aspects of assessing tumors using clinical diffusion-weighted imaging in the body. Magn Reson Med Sci 2007; 6: pp. 211-224.
21. Ohno Y., Koyama H., Onishi Y., et. al.: Non-small cell lung cancer: whole-body MR examination for M-stage assessment–utility for whole-body diffusion-weighted imaging compared with integrated FDG PET/CT. Radiology 2008; 248: pp. 643-654.
22. Vilanova J.C., Barcelo J.: Diffusion-weighted whole-body MR screening. Eur J Radiol 2008; 67: pp. 440-447.
23. Heusner T.A., Kuemmel S., Koeninger A., et. al.: Diagnostic value of diffusion-weighted magnetic resonance imaging (DWI) compared to FDG PET/CT for whole-body breast cancer staging. Eur J Nucl Med Mol Imaging 2010; 37: pp. 1077-1086.
24. Lin C., Itti E., Luciani A., et. al.: Whole-body diffusion-weighted imaging with apparent diffusion coefficient mapping for treatment response assessment in patients with diffuse large B-cell lymphoma: pilot study. Invest Radiol 2011; 46: pp. 341-349.
25. Schmidt G.P., Baur-Melnyk A., Haug A., et. al.: Comprehensive imaging of tumor recurrence in breast cancer patients using whole-body MRI at 1.5 and 3 T compared to FDG-PET-CT. Eur J Radiol 2008; 65: pp. 47-58.
26. Fayad L.M., Blakeley J., Plotkin S., et. al.: Whole body MRI at 3T with quantitative diffusion weighted imaging and contrast-enhanced sequences for the characterization of peripheral lesions in patients with neurofibromatosis type 2 and schwannomatosis. ISRN Radiol 2013; 2013: pp. 9.
27. Ahlawat S., Baig A., Blakeley J.O., et. al.: Multiparametric whole-body anatomic, functional, and metabolic imaging characteristics of peripheral lesions in patients with schwannomatosis. J Magn Reson Imaging 2016; 44: pp. 794-803.
28. Schweitzer M.E., Levine C., Mitchell D.G., et. al.: Bull’s-eyes and halos: useful MR discriminators of osseous metastases. Radiology 1993; 188: pp. 249-252.
29. Mirowitz S.A., Apicella P., Reinus W.R., et. al.: MR imaging of bone marrow lesions: relative conspicuousness on T1-weighted, fat-suppressed T2-weighted, and STIR images. Am J Roentgenol 1994; 162: pp. 215-221.
30. Thie J.A.: Understanding the standardized uptake value, its methods, and implications for usage. J Nucl Med 2004; 45: pp. 1431-1434.
31. Wahl R.L., Jacene H., Kasamon Y., et. al.: From RECIST to PERCIST: evolving considerations for PET response criteria in solid tumors. J Nucl Med 2009; 50: pp. 122S-150S.
32. Yoshikawa T., Kawamitsu H., Mitchell D.G., et. al.: ADC measurement of abdominal organs and lesions using parallel imaging technique. Am J Roentgenol 2006; 187: pp. 1521-1530.
33. Yuan Z., Ye X.D., Dong S., et. al.: Role of magnetic resonance diffusion-weighted imaging in evaluating response after chemoembolization of hepatocellular carcinoma. Eur J Radiol 2010; 75: pp. e9-e14.
34. Eiber M., Holzapfel K., Ganter C., et. al.: Whole-body MRI including diffusion-weighted imaging (DWI) for patients with recurring prostate cancer: technical feasibility and assessment of lesion conspicuity in DWI. J Magn Reson Imaging 2011; 33: pp. 1160-1170.
35. Vermathen P., Binser T., Boesch C., et. al.: Three-year follow-up of human transplanted kidneys by diffusion-weighted MRI and blood oxygenation level-dependent imaging. J Magn Reson Imaging 2012; 35: pp. 1133-1138.
36. Lavdas I., Rockall A.G., Castelli F., et. al.: Apparent diffusion coefficient of normal abdominal organs and bone marrow from whole-body DWI at 1.5 T: the effect of sex and age. Am J Roentgenol 2015; 205: pp. 242-250.
37. Oner A.Y., Aggunlu L., Akpek S., et. al.: Diffusion-weighted imaging of the appendicular skeleton with a non-Carr-Purcell-Meiboom-Gill single-shot fast spin-echo sequence. Am J Roentgenol 2007; 189: pp. 1494-1501.
38. Yang H.L., Liu T., Wang X.M., et. al.: Diagnosis of bone metastases: a meta-analysis comparing (1)(8)FDG PET, CT, MRI and bone scintigraphy. Eur Radiol 2011; 21: pp. 2604-2617.
39. Lecouvet F.E., El Mouedden J., Collette L., et. al.: Can whole-body magnetic resonance imaging with diffusion-weighted imaging replace Tc 99m bone scanning and computed tomography for single-step detection of metastases in patients with high-risk prostate cancer?. Eur Urol 2012; 62: pp. 68-75.
40. Shen G., Deng H., Hu S., et. al.: Comparison of choline-PET/CT, MRI, SPECT, and bone scintigraphy in the diagnosis of bone metastases in patients with prostate cancer: a meta-analysis. Skeletal Radiol 2014; 43: pp. 1503-1513.
41. Pasoglou V., Michoux N., Peeters F., et. al.: Whole-body 3D T1-weighted MR imaging in patients with prostate cancer: feasibility and evaluation in screening for metastatic disease. Radiology 2015; 275: pp. 155-166.
42. Wahl R.L.: Positron emission tomography (PET): an update on applications in breast cancer. Breast Dis 1998; 10: pp. 165-175.
43. Reske S.N., Blumstein N.M., Neumaier B., et. al.: Imaging prostate cancer with 11C-choline PET/CT. J Nucl Med 2006; 47: pp. 1249-1254.
44. Chen X., Moore M.O., Lehman C.D., et. al.: Combined use of MRI and PET to monitor response and assess residual disease for locally advanced breast cancer treated with neoadjuvant chemotherapy. Acad Radiol 2004; 11: pp. 1115-1124.
45. Judenhofer M.S., Wehrl H.F., Newport D.F., et. al.: Simultaneous PET-MRI: a new approach for functional and morphological imaging. Nat Med 2008; 14: pp. 459-465.
46. Uematsu T., Kasami M., Yuen S.: Comparison of FDG PET and MRI for evaluating the tumor extent of breast cancer and the impact of FDG PET on the systemic staging and prognosis of patients who are candidates for breast-conserving therapy. Breast Cancer 2009; 16: pp. 97-104.
47. Jacobs M.A., Wolff A., Ouwerkerk R., et. al.: Monitoring of neoadjuvant chemotherapy using multiparametric, (23)Na sodium MR, and multimodality (PET/CT/MRI) imaging in locally advanced breast cancer. Breast Cancer Res Treat 2011; 128: pp. 119-126.
48. Antoch G., Bockisch A.: Combined PET/MRI: a new dimension in whole-body oncology imaging?. Eur J Nucl Med Mol Imaging 2009; 36: pp. S113-S120.
49. Buchbender C., Heusner T.A., Lauenstein T.C., et. al.: Oncologic PET/MRI, part 1: tumors of the brain, head and neck, chest, abdomen, and pelvis. J Nucl Med 2012; 53: pp. 928-938.
50. Buchbender C., Heusner T.A., Lauenstein T.C., et. al.: Oncologic PET/MRI, part 2: bone tumors, soft-tissue tumors, melanoma, and lymphoma. J Nucl Med 2012; 53: pp. 1244-1252.