
Rationale and Objectives
To investigate the value of multiplanar reconstructions (MPRs) of automated three-dimensional (3D) breast ultrasound (ABUS) compared to transverse evaluation only, in differentiation of benign and malignant breast lesions.
Materials and Methods
Five breast radiologists evaluated ABUS scans of 96 female patients with biopsy-proven abnormalities (36 malignant and 60 benign). They classified the most suspicious lesion based on the breast imaging reporting and data system (BI-RADS) lexicon using the transverse scans only. A likelihood-of-malignancy (LOM) score (0–100) and a BI-RADS final assessment were assigned. Thereafter, the MPR was provided and readers scored the cases again. In addition, they rated the presence of spiculation and retraction in the coronal plane on a five-point scale called Spiculation and Retraction Severity Index (SRSI). Reader performance was analyzed with receiver-operating characteristics analysis.
Results
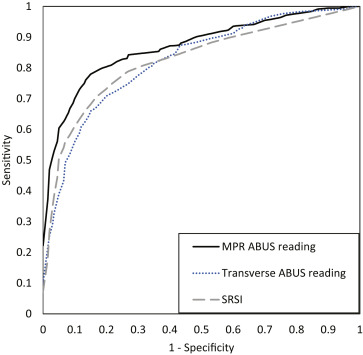
The area under the curve increased from 0.82 to 0.87 ( P = .01) after readers were shown the reconstructed planes. The SRSI scores are highly correlated (Spearman’s r ) with the final LOM scores (range, r = 0.808–0.872) and ΔLOM scores (range, r = 0.525–0.836). Readers downgraded 3%–18% of the biopsied benign lesions to BI-RADS 2 after MPR evaluation. Inter-reader agreement for SRSI was substantial (intraclass correlation coefficient, 0.617). Inter-reader agreement of the BI-RADS final assessment improved from 0.367 to 0.536 after MPRs were read.
Conclusions
Full 3D evaluation of ABUS using MPR improves differentiation of breast lesions in comparison to evaluating only transverse planes. Results suggest that the added value of MPR might be related to visualization of spiculation and retraction patterns in the coronal reconstructions.
Handheld ultrasound (HHUS) is a standard diagnostic modality in breast cancer diagnosis. HHUS is also increasingly used for screening because of the increasing awareness of underperformance of mammography in women with dense breasts. Additional screening with bilateral whole breast HHUS in these women improves the cancer detection rate . However, HHUS whole breast screening is time consuming and should be performed by a trained physician. HHUS is therefore relatively expensive. Automated three-dimensional (3D) breast ultrasound (ABUS) can overcome these limitations of HHUS. The acquisition is performed by a technician who positions the automatically driven wide linear array transducer for each volume on a predefined location of the breast. Depending on the size of the breast, three–five separate ABUS volumes are required for full breast coverage . The acquisition of standardized volumes enables comparison of new examinations to relevant priors, which is not feasible with HHUS.
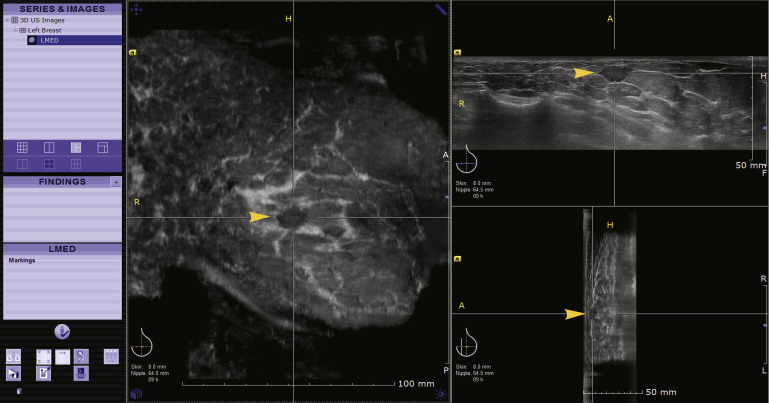
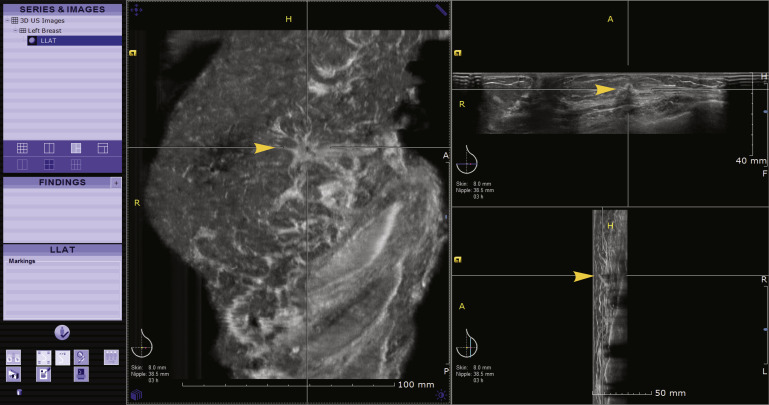
ABUS volume scans consist of a series of sequential transverse images. These are reconstructed into coronal and sagittal images on a dedicated workstation ( Fig 1 ). Coronal reconstructions provide a comprehensive view of the breast anatomy and visualize the effect of breast lesions on neighboring breast tissue . Spiculation of malignant lesions and the retraction phenomenon caused by an accompanying desmoplastic reaction give rise to architectural distortion, which is best viewed in this coronal plane . The architectural distortion discriminates strongly between benign and malignant breast lesions .
 Open full size image
Open full size image
Figure 1
Multiplanar reconstructions of automated breast ultrasound (ABUS) and reading protocol. The original transverse ABUS images are reconstructed into coronal and sagittal planes. The reader can therefore view the breast lesion in three orthogonal planes (eg transverse, coronal, and sagittal). The coronal reconstructions provide a comprehensive view on the breast anatomy. During the reader experiment, the readers initially were shown the transverse images only on full screen (top plane of this figure only) to classify the most suspicious lesion. Thereafter, the MPRs were shown and readers were asked to classify the lesion again and rate spiculation and retraction in the coronal plane. (Color version of figure is available online.)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Methods
Get Radiology Tree app to read full this article<
Inclusion and Exclusion of Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Gold Standard
Get Radiology Tree app to read full this article<
ABUS Examination
Get Radiology Tree app to read full this article<
Readers
Get Radiology Tree app to read full this article<
Patient Characteristics
Get Radiology Tree app to read full this article<
Table 1
Characteristics of Malignant Lesions
Pathology Results Median Lesion Size in mm (Range) Invasive ductal carcinoma (n = 6) 19 (13–40) Invasive ductal carcinoma, ductal carcinoma in situ combined (n = 22) 19.5 (7.5–70) Invasive lobular carcinoma (n = 6) 30 (17–130) Papillary carcinoma (n = 2) 18.5 (15–22)
A total of 36 cases showed a malignant lesion with a variety of cancer types and sizes. All malignant lesions were biopsied under ultrasound guidance.
Table 2
Characteristics of Benign Lesions
Pathology Results Median Lesion Size in mm (Range) Infectious lesion (n = 6) 15 (5–25) Fibroadenoma (n = 21) 10 (6–18) Complex cysts (n = 5) 10 (6–25) Adenosis (tumor; n = 3) 8 (5–20) Fibrosis (n = 6) 20 (8–40) Intraductal papilloma (n = 5) 12 (4–18) Hamartoma (n = 1) 16 Clustered microcysts (n = 3) 10 (10–16) Complex sclerosing lesions (n = 3) 20 (15–44) Fasciitis nodularis (n = 1) 8 Atypical inflammation (n = 6) 8 (5–17)
Sixty cases showed lesions that were proven benign with a variety lesion types and sizes. All benign lesions were biopsied under ultrasound guidance.
Get Radiology Tree app to read full this article<
Methodology of ABUS Reading
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Reader Performance
Get Radiology Tree app to read full this article<
Table 3
Areas Under the Curve After Transverse Reading, Multiplanar Reconstructions Reading, and Based on SRSI Values
Reader Transverse AUC SE MPR AUC SE SRSI AUC SE 1 0.881 0.038 0.907 0.034 0.883 0.036 2 0.852 0.039 0.884 0.036 0.828 0.047 3 0.826 0.044 0.897 0.036 0.796 0.052 4 0.743 0.054 0.818 0.049 0.797 0.051 5 0.829 0.044 0.854 0.045 0.824 0.045 Average 0.826 0.039 0.872 0.035 0.825 0.034
AUC, area under the receiver-operating characteristic curve; MPR, multiplanar reconstruction; SE, standard error; SRSI, Spiculation and Retraction Severity Index.
The AUC for each radiologist before and after the evaluation of MPRs. All radiologists improve differentiation between benign and malignant lesions. Overall performance increased significantly. Averaged AUC of SRSI is almost equal to the averaged AUC after transverse reading.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Spiculation and Retraction Severity Index
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Reader Agreement
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Berg W.A., Blume J.D., Cormack J.B., et. al.: Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer. JAMA. American Medical Association 2008; 299: pp. 2151-2163.
2. Buchberger W., Niehoff A., Obrist P., et. al.: Clinically and mammographically occult breast lesions: detection and classification with high-resolution sonography. Semin Ultrasound, CT MRI 2000; 21: pp. 325-336.
3. Kolb T.M., Lichy J., Newhouse J.H.: Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology. Radiological Society of North America 2002; 225: pp. 165-175.
4. Bae M.S., Moon W.K., Chang J.M., et. al.: Breast cancer detected with screening US: reasons for nondetection at mammography. Radiology 2014; 270: pp. 369-377.
5. Wojcinski S., Farrokh A., Hille U., et. al.: The Automated Breast Volume Scanner (ABVS): initial experiences in lesion detection compared with conventional handheld B-mode ultrasound: a pilot study of 50 cases. Int J Womens Heal 2011; 3: pp. 337-346.
6. Tozaki M., Isobe S., Yamaguchi M., et. al.: Optimal scanning technique to cover the whole breast using an automated breast volume scanner. Jpn J Radiol 2010; 28: pp. 325-328.
7. Wang H.Y., Jiang Y.X., Zhu Q.L., et. al.: Differentiation of benign and malignant breast lesions: a comparison between automatically generated breast volume scans and handheld ultrasound examinations. Eur J Radiol 2012; 81: pp. 3190-3200.
8. Zhang J., Lai X.J., Zhu Q.L., et. al.: Interobserver agreement for sonograms of breast lesions obtained by an automated breast volume scanner. Eur J Radiol 2012; 81: pp. 2179-2183.
9. Chen L., Chen Y., Diao X.H., et. al.: Comparative study of automated breast 3-D ultrasound and handheld B-mode ultrasound for differentiation of benign and malignant breast masses. Ultrasound Med Biol 2013; 39: pp. 1735-1742.
10. Lin X., Wang J., Han F., et. al.: Analysis of eighty-one cases with breast lesions using automated breast volume scanner and comparison with handheld ultrasound. Eur J Radiol 2012; 81: pp. 873-878.
11. Kotsianos-Hermle D., Hiltawsky K.M., Wirth S., et. al.: Analysis of 107 breast lesions with automated 3D ultrasound and comparison with mammography and manual ultrasound. Eur J Radiol 2009; 71: pp. 109-115.
12. Rotten D., Levaillant J.M., Zerat L.: Analysis of normal breast tissue and of solid breast masses using three-dimensional ultrasound mammography. Ultrasound Obstet Gynecol 1999; 14: pp. 114-124.
13. Stavros A.T., Thickman D., Rapp C.L., et. al.: Solid breast nodules: use of sonography to distinguish between benign and malignant lesions. Radiology 1995; 196: pp. 123-134.
14. Golatta M., Franz D., Harcos A., et. al.: Interobserver reliability of automated breast volume scanner (ABVS) interpretation and agreement of ABVS findings with hand held breast ultrasound (HHUS), mammography and pathology results. Eur J Radiol 2013; 82: pp. 332-336.
15. Lazarus E., Mainiero M.B., Schepps B., et. al.: BI-RADS lexicon for US and mammography: interobserver variability and positive predictive value. Radiology. Radiological Society of North America 2006; 239: pp. 385-391.
16. Abdullah N., Mesurolle B., El-Khoury M., et. al.: Breast imaging reporting and data system lexicon for US: interobserver agreement for assessment of breast masses. Radiology. Radiological Society of North America, Inc 2009; 252: pp. 665-672.
17. Berg W.A., Blume J.D., Cormack J.B., et. al.: Operator dependence of physician-performed whole-breast US: lesion detection and characterization. Radiology. Radiological Society of North America 2006; 241: pp. 355-365.
18. Lee H.J., Kim E.K., Kim M.J., et. al.: Observer variability of Breast Imaging Reporting and Data System (BI-RADS) for breast ultrasound. Eur J Radiol 2008; 65: pp. 293-298.
19. Nothacker M., Duda V., Hahn M., et. al.: Early detection of breast cancer: benefits and risks of supplemental breast ultrasound in asymptomatic women with mammographically dense breast tissue. A systematic review. BMC Cancer 2009; 9: pp. 335.
20. Brem R.F., Tabár L., Duffy S.W., et. al.: Assessing improvement in detection of breast cancer with three-dimensional automated breast US in women with dense breast tissue: the SomoInsight Study. Radiology 2015; 274: pp. 663-673.
21. Schalekamp S., van Ginneken B., Schaefer-Prokop C.M., et. al.: Influence of study design in receiver operating characteristics studies: sequential versus independent reading. J Med Imaging. International Society for Optics and Photonics 2014; 1: pp. 015501.
22. Beiden S.V., Wagner R.F., Doi K., et. al.: Independent versus sequential reading in ROC studies of computer-assist modalities: analysis of components of variance. Acad Radiol 2002; 9: pp. 1036-1043.
23. Kelly K.M., Dean J., Comulada W.S., et. al.: Breast cancer detection using automated whole breast ultrasound and mammography in radiographically dense breasts. Eur Radiol 2010; 20: pp. 734-742.
24. Sedgwick E.: The breast ultrasound lexicon: breast imaging reporting and data system (BI-RADS). Semin Roentgenol 2011; 46: pp. 245-251.
25. Levy L., Suissa M., Chiche J.F., et. al.: BIRADS ultrasonography. Eur J Radiol 2007; 61: pp. 202-211.
26. Mendelson E.B., Berg W.A., Merritt C.R.: Toward a standardized breast ultrasound lexicon, BI-RADS: ultrasound. Semin Roentgenol 2001; 36: pp. 217-225.
27. Jiang Y., Metz C.E.: BI-RADS data should not be used to estimate ROC curves. Radiology 2010; 256: pp. 29-31.
28. Wagner R.F., Beiden S.V., Metz C.E.: Continuous versus categorical data for ROC analysis: some quantitative considerations. Acad Radiol 2001; 8: pp. 328-334.
29. Metz C.E.: ROC methodology in radiologic imaging. Invest Radiol 1986; 21: pp. 720-733.
30. Metz C.E., Herman B.A., Roe C.A.: Statistical comparison of two ROC-curve estimates obtained from partially-paired datasets. Med Decis Mak 1998; 18: pp. 110-121.
31. Dorfman D.D., Berbaum K.S., Metz C.E.: Receiver operating characteristic rating analysis: generalization to the population of readers and patients with the jackknife method. Invest Radiol 1992; 27: pp. 723-731.
32. Hillis S.L., Berbaum K.S., Metz C.E.: Recent developments in the Dorfman-Berbaum-Metz procedure for multireader ROC study analysis. Acad Radiol 2008; 15: pp. 647-661.
33. Spearman C.: The proof and measurement of association between two things. By C. Spearman, 1904. Am J Psychol 1987; 100: pp. 441-471.
34. Wang Z.L., Xu J.H., Xw J.H., et. al.: Comparison of automated breast volume scanning to hand-held ultrasound and mammography. Radiol Med 2012; 117: pp. 1287-1293.
35. Zhang Q., Hu B., Li W.B.: Detection of breast lesions using an automated breast volume scanner system. J Int Med Res 2012; 40: pp. 300-306.
36. Mendelson : ACR practice guideline for the performance of a breast ultrasound examination.2011. Revised 2011 (Resolution 11)
37. Franquet T., De Miguel C., Cozcolluela R., et. al.: Spiculated lesions of the breast: mammographic-pathologic correlation. Radiographics. American Public Health Association 1993; 13: pp. 841-852.
38. Jacobs T.W., Byrne C., Colditz G., et. al.: Radial scars in benign breast-biopsy specimens and the risk of breast cancer. N Engl J Med 1999; 340: pp. 430-436.