
Rationale and Objectives
The clinical utility of supine in-magnet bicycling in combination with phosphorus magnetic resonance spectroscopy ( 31 P MRS) to evaluate quadriceps muscle metabolism was examined in four children with juvenile dermatomyositis (JDM) in remission and healthy age- and gender-matched controls.
Materials and Methods
Two identical maximal supine bicycling tests were performed using a magnetic resonance–compatible ergometer. During the first test, cardiopulmonary performance was established in the exercise laboratory. During the second test, quadriceps energy balance and acid/base balance during incremental exercise and phosphocreatine recovery were determined using 31 P MRS.
Results
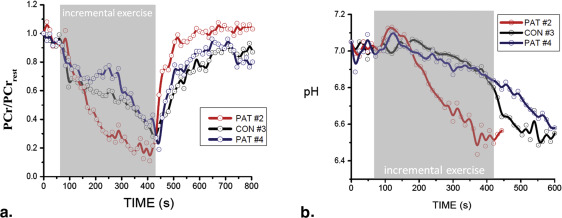
During the first test, no significant differences were found between patients with JDM and their healthy peers regarding cardiopulmonary performance. The outcomes of the first test indicate that both groups attained maximal performance. During the second test, quadriceps phosphocreatine and pH time courses were similar in all but one patient experiencing idiopathic postexercise pain. This patient demonstrated faster phosphocreatine depletion and acidification during exercise, yet postexercise mitochondrial adenosine triphosphate synthesis rate measured by phosphocreatine recovery kinetics was approximately twofold faster than control (time constant 23 seconds vs 43 ± 7 seconds, respectively).
Conclusions
These results highlight the utility of in-magnet cycle ergometry in combination with 31 P MRS to assess and monitor muscle energetic patterns in pediatric patients with inflammatory myopathies.
Exercise is increasingly used as a nonpharmacological intervention in the clinical management of patients with chronic inflammatory conditions. Evaluation of the impact of exercise on systemic health commonly involves periodic testing with concomitant measurement of direct and indirect physiological outcome parameters (eg, maximal oxygen uptake) . These, however, are all macroscopic outcome measures that greatly rely on voluntary effort. Availability of more objective outcome measures that provide functional information at the cellular, or even molecular, level would significantly strengthen ongoing efforts to tailor exercise interventions to individual patient needs and limitations. Although muscle biopsies before and after exercise may provide relevant microscopic information , the procedure is highly invasive and therefore undesirable, particularly in pediatric care. Therefore, we explored the potential of an in vivo magnetic resonance (MR)–based methodology to serve as a sensitive and noninvasive tool that guides the development of personalized exercise interventions.
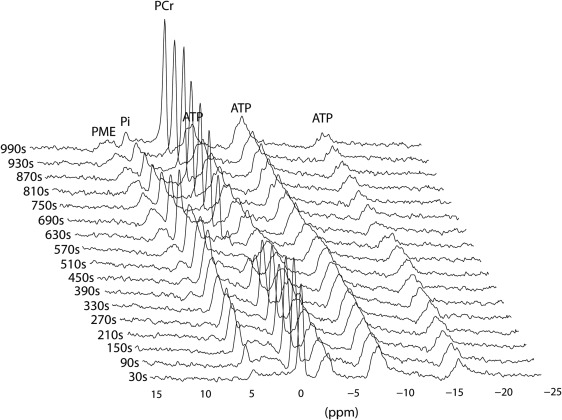
In vivo phosphorus magnetic resonance spectroscopy ( 31 P MRS) has long offered a noninvasive window into the metabolic capacity of skeletal muscle to support exercise . Recordings of 31 P MR spectra from human muscle during exercise and metabolic recovery have been commonly used to evaluate cellular adenosine triphosphate (ATP) synthetic function on the basis of dynamic changes in phosphocreatine (PCr), inorganic phosphate (Pi), and intracellular pH . In a more general sense, these recordings yield information on the in vivo homeostatic capacity of the metabolic networks in muscle with respect to myocellular energy balance (MEB) and myocellular proton balance (MPB) during exercise.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Subjects
Get Radiology Tree app to read full this article<
Ergometer
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Cardiopulmonary Exercise Testing (CPET)
Get Radiology Tree app to read full this article<
Table 1
Anthropometrics and Measurements During the First CPET (Outside MRS) Including Gas Analysis
Demographic Children with JDM in Remission ( N = 4); Median (Range) Children in the Control Group ( N = 3); Median (Range) Significance (Two Tailed) Age (years) 15.7 (3.5) 15.5 (2.6) 0.71 Height (cm) 169.5 (21.0) 180.5 (26.5) 0.86 Weight (kg) 60.6 (20.4) 67.7 (24.9) 0.86 BMI (kg/m 2 ) 20.6 (3.0) 19.7 (3.6) 0.86 HR peak (bpm) 182 (19.0) 187 (30.0) 1.00 RER peak 1.05 (0.07) 1.04 (0.23) 0.94 VO 2peak (L/min) 2.23 (1.9) 2.75 (1.4) 0.63 VO 2peak/kg (mL/kg/min) 35.9 (24.4) 38.8 (10.5) 0.63 Peak work load (kg) 2.9 (2.3) 2.3 (1.8) 0.97 VO 2 /HR peak 12.5 (9.4) 14.1 (6.5) 0.86
BMI, body mass index; CPET, cardiopulmonary exercise test; MRS, magnetic resonance spectroscopy; RER, respiratory exchange ratio; VCO 2 , carbon dioxide production; VO 2 , oxygen uptake.
Get Radiology Tree app to read full this article<
1 H and 31 P MRS
Get Radiology Tree app to read full this article<
Statistics and Data Processing
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Wasserman K., Hanssen J.E., Sue D.Y., et. al.: Principles of exercise testing and interpretation.4th ed.2005.Lippincott Williams & WilkinsPhiladelphia, PA
2. Constatin-Teodosiu D., Casey A., Short A.H., et. al.: The effect of repeated muscle biopsy sampling on ATP and glycogen resynthesis following exercise in man. Eur J Appl Physiol Occup Physiol 1996; 73: pp. 186-190.
3. Chance B., Im J., Nioka S., et. al.: Skeletal muscle energetics with PNMR: personal views and historic perspectives. NMR Biomed 2006; 19: pp. 904-926.
4. Jeneson J.A., Bruggeman F.J.: Robust homeostatic control of quadriceps pH during natural locomotor activity in man. FASEB J 2004; 18: pp. 1010-1012.
5. Taylor D.J., Bore P.J., Styles P., et. al.: Bioenergetics of intact human muscle. A31P nuclear magnetic resonance study. Mol Biol Med 1983; 1: pp. 77-94.
6. Jeneson J.A., Schmitz J.P., Hilbers P.A., et. al.: An MR-compatible bicycle ergometer for in- magnet whole-body human exercise testing. Magn Reson Med 2010; 63: pp. 257-261.
7. Rider L.G., Miller F.W.: Classification and treatment of the juvenile idiopathic inflammatory myopathies. Rheum Dis Clin North Am 1997; 23: pp. 619-655.
8. Feldman B.M., Rider L.G., Reed A.M., et. al.: Juvenile dermatomyositis and other idiopathic inflammatory myopathies of childhood. Lancet 2008; 371: pp. 2201-2212.
9. Takken T., van der Net J., Engelbert R.H., et. al.: Responsiveness of exercise parameters in children with inflammatory myositis. Arthritis Rheum 2008; 59: pp. 59-64.
10. Prompers J.J., Jeneson J.A., Drost M.R., et. al.: Dynamic MRS and MRI of skeletal muscle function and biomechanics. NMR Biomed 2006; 19: pp. 927-953. Review
11. Van den Broek N.A.M., de Feyter H.M., de Graaf L., et. al.: Intersubject differences in the effect of acidosis on phosphocreatine recovery in exercise are due to differences in proton efflux rates. Am J Physiol Cell Physiol 2007; 293: pp. C228-C237.
12. Cea G., Bendahan D., Manners D., et. al.: Reduced oxidative phosphorylation and proton efflux suggest reduced capillary blood supply in skeletal muscle of patients with dermatomyositis and polymyositis: a quantitative 31P-magnetic resonance spectroscopy and MRI study. Brain 2002; 125: pp. 1635-1645.
13. Park J.H., Vansant J.P., Kumar N.G., et. al.: Dermatomyositis: correlative MR imaging and P-31 MR spectroscopy for quantitative characterization of inflammatory disease. Radiology 1990; 177: pp. 473-479.
14. Park J.H., Niermann K.J., Ryder N.M., et. al.: Muscle abnormalities in juvenile dermatomyositis patients: P-31 Magnetic Resonance Spectroscopy studies. Arthritis Rheum 2000; 43: pp. 2359-2367.
15. Park J.H., Olsen N.J.: Utility of magnetic resonance imaging in the evaluation of patients with inflammatory myopathies. Curr Rheumatol Rep 2001; 3: pp. 334-345.
16. Pfleiderer B., Lange J., Loske K.D., et. al.: Metabolic disturbances during short exercises in dermatomyositis revealed by real-time functional 31P magnetic resonance spectroscopy. Rheumatology 2004; 43: pp. 696-703.
17. Niermann K.J., Olsen N.J., Park J.H.: Magnesium abnormalities of skeletal muscle in dermatomyositis and juvenile dermatomyositis. Arthritis Rheum 2002; 46: pp. 475-488.
18. Park J.H., Kari S., King L.E., et. al.: Analysis of 31P MR spectroscopy data using artificial neural networks for longitudinal evaluation of muscle diseases: dermatomyositis. NMR Biomed 1998; 11: pp. 245-256.
19. Slopis J.M., Jackson E.F., Narayana P.A., et. al.: Proton magnetic resonance imaging and spectroscopic studies of the pathogenesis and treatment of juvenile dermatomyositis. J Child Neurol 1993; 8: pp. 242-249.
20. Takken T., Elst E.F., van der Net J.: Pathophysiological factors which determine the exercise intolerance in patients with juvenile dermatomyositis. Curr Rheumatol Rev 2005; 1: pp. 91-99.