
Rationale and Objectives
The aim of this prospective, randomized animal study was to compare a new computer guided needle–based navigation system for liver biopsy with conventional computed tomography (CT)-guided liver biopsy. Computer-navigated interventions provide continuous needle tracking during motion and deformation from patient respiration and movement.
Materials and Methods
Twenty artificial tumors of about 5 mm in diameter were injected into the livers of five pigs, each at a different site. Each tumor was targeted by conventional CT-guided and computer navigated intervention. Intervention was considered complete after successful tumor biopsy. Data on procedure time, number of CT scans performed, accuracy, and success rate were recorded.
Results
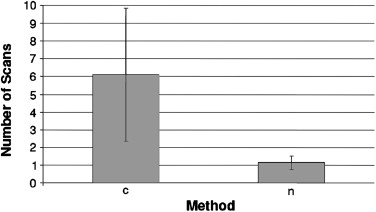
All tumors (100%) were biopsied successfully. Mean procedural time was comparable between the two techniques (20 ± 9 minutes conventional versus 20 ± 8 minutes navigation). Mean number of CT scans were 1.2 ± 0.4 with navigation and 6.1 ± 3.8 with the conventional technique ( P < .01). The dose-length product in the conventional group was significantly higher (212 ± 116 mGy × cm) than in the navigated group (78 ± 22 mGy × cm; P < .001). Mean number of capsule penetrations was 4 ± 1 with navigation versus 2 ± 1 with the conventional technique ( P < .001).
Conclusion
Computer-navigated liver biopsy may provide a promising and innovative device for easy, rapid, and successful liver biopsies with low morbidity. Further technical improvements and clinical studies in humans are required.
Convergent developments in radiology, teletransmission, computer science, and surgical innovations have allowed for the development of image-guided surgery and navigation. These techniques are well-established in the daily routine in orthopedic, neuro-, and head and neck surgery for improving precision and minimizing radiation exposure . However, the use of computer navigation systems for interventions in soft organs with motion and deformation, such as the liver is not yet established and constitutes an area of current research .
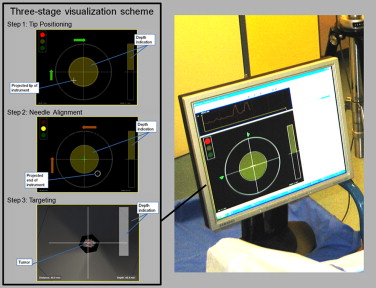
In cooperation with the German Cancer Research Center (Heidelberg, Germany), an image-guided navigation system was developed using optical tracking including fiducial needles in combination with preprocedural computer tomography (CT) imaging. After promising results with in vitro studies , we examined common clinical procedures in the liver to select a clinical relevant standardized procedure to evaluate technical aspects of computer navigation and allow comparison to current clinical practice . Based on this examination, we chose to evaluate CT-guided liver biopsy with and without the use of our novel soft-tissue navigation system.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Experimental Setting, Artificial Tumor Placement, and Parameters
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conventional CT-guided Liver Biopsy
Get Radiology Tree app to read full this article<
Navigated Liver Biopsy
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Comparative Data of Both the Conventional and the Navigated Group
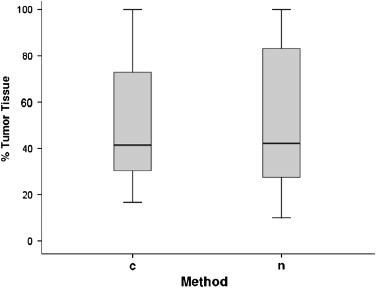
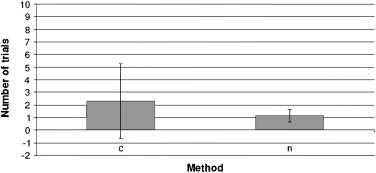
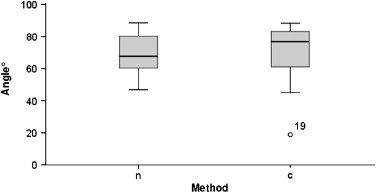
Parameter Conventional Liver Biopsy Navigated Liver Biopsy_P_ Overall procedure time (minutes) 20 ± 9 20 ± 8 .8 Mean number of computed tomography scans 6.1 ± 3.8 1.2 ± 0.4 <.01 Dose length product (mGy × cm) 212 ± 116 78 ± 22 <.001 Extracted tumor tissue (%) 53 ± 31 51 ± 29 .87 First pass accuracy (%) 94 ± 18 74 ± 32 <.05 Mean number of trials 2.3 ± 2.9 1.2 ± 0.5 <.05 Number of attempts to target tumor 3.0 ± 3.0 1.0 ± 0 <.001 Needle repositioning 3.2 ± 3.8 0.2 ± 0.5 <.001 Liver capsule penetration 2.0 ± 1.0 4.0 ± 1.0 <.001 Angle of the needle 70.1 ± 17.3 69 ± 12.7 >.5
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Nolte L.P., Slomczykowski M.A., Berlemann U., et. al.: A new approach to computer-aided spine surgery: fluoroscopy-based surgical navigation. Eur Spine 2000; 9: pp. 78-88.
2. Schiemann M., Killmann R., Kleen M., et. al.: Vascular guide wire navigation with a magnetic guidance system: Experimental results in a phantom. Radiology 2004; 232: pp. 475-481.
3. Biasca N., Schneider T.O., Bungartz M.: Minimally invasive computer-navigated total knee arthroplasty. Orthop Clin North Am 2009; 40: pp. 537-563.
4. Clifford M.A., Banovac F., Levy E., et. al.: Assessment of hepatic motion secondary to respiration for computer assisted interventions. Comput Aided Surg 2002; 7: pp. 291-299.
5. Khan M.F., Dogan S., Maataoui A., et. al.: Navigation-based needle puncture of a cadaver using a hybrid tracking navigational system. Invest Radiol 2006; 41: pp. 713-720.
6. Banovac F., Tang J., Xu S., et. al.: Precision targeting of liver lesions using a novel electromagnetic navigation device in physiologic phantom and swine. Med Phys 2005; 32: pp. 2698-2705.
7. Maier-Hein L., Pianka F., Seitel A., et. al.: Precision targeting of liver lesions with a needle-based soft tissue navigation system. Med Image Comput Comput Assist Interv Int Conf Med Image Comput Comput Assist Interv 2007; 10: pp. 42-49.
8. Fichtinger G., Deguet A., Fischer G., et. al.: Image overlay for CT-guided needle insertions. Comput Aided Surg 2005; 10: pp. 241-255.
9. Zhang H., Banovac F., Lin R., et. al.: Electromagnetic tracking for abdominal interventions in computer aided surgery. Comput Aided Surg 2006; 11: pp. 127-136.
10. Krücker J., Xu S., Glossop N., et. al.: Electromagnetic tracking for thermal ablation and biopsy guidance: clinical evaluation of spatial accuracy. J Vasc Interv Radiol 2007; 18: pp. 1141-1150.
11. Maier-Hein L., Tekbas A., Seitel A., et. al.: In vivo accuracy assessment of a needle-based navigation system for CT-guided radiofrequency ablation of the liver. Med Phys 2008; 35: pp. 5385-5396.
12. Maier-Hein L., Müller S.A., Pianka F., et. al.: Respiratory motion compensation for CT-guided interventions in the liver. Comput Aided Surg 2008; 13: pp. 125-138.
13. Müller S.A., Maier-Hein L., Mehrabi A., et. al.: Creation and establishment of a respiratory liver motion simulator for liver interventions. Med Phys 2007; 34: pp. 4605-4608.
14. Maier-Hein L., Tekbas A., Franz A.M., et. al.: On combining internal and external fiducials for liver motion compensation. Comput Aided Surg 2008; 13: pp. 369-376.
15. Welch T.J., Sheedy P.F., Johnson C.D., et. al.: CT-guided biopsy: prospective analysis of 1,000 procedures. Radiology 1989; 171: pp. 493-496.
16. Copel L., Sosna J., Kruskal J.B., et. al.: Ultrasound-guided percutaneous liver biopsy: indications, risks, and technique. Surg Technol Int 2003; 11: pp. 154-160.
17. Wallace M.J., Gupta S., Hicks M.E.: Out-of-plane computed-tomography-guided biopsy using a magnetic-field-based navigation system. Cardiovasc Intervent Radiol 2006; 29: pp. 108-113.
18. Yu S.C., Liew C.T., Lau W.Y., et. al.: US-guided percutaneous biopsy of small (< or = 1-cm) hepatic lesions. Radiology 2001; 218: pp. 195-199.
19. Middleton W.D., Hiskes S.K., Teefey S.A., et. al.: Small (1.5 cm or less) liver metastases: US-guided biopsy. Radiology 1997; 205: pp. 729-732.
20. Golling M., Kellner H., Fonouni H., et. al.: Reduced glutathione in the liver as a potential viability marker in non-heart-beating donors. Liver Transpl 2008; 14: pp. 1637-1647.
21. Müller-Stich B.P., Mehrabi A., Kenngott H.G., et. al.: Improved reflux monitoring in the acute gastroesophageal reflux porcine model using esophageal multichannel intraluminal impedance measurement. J Gastrointest Surg 2008; 12: pp. 1351-1358.
22. Court F.G., Wemyss-Holden S.A., Morrison C.P., et. al.: Segmental nature of the porcine liver and its potential as a model for experimental partial hepatectomy. Br J Surg 2003; 90: pp. 440-444.
23. Seitel A., Maier-Hein L., Schawo S., et. al.: In-vitro evaluation of different visualization approaches for computer assisted targeting in soft tissue. Int J CARS 2007; 2: pp. 188-190.
24. Tekbas A, Maier-Hein L, Müller SA, et al. Technical implementation of a new computer assisted navigation system for percutaneous liver biopsy—pitfalls and potential benefits. (in preparation)
25. Wood B.J., Zhang H., Durrani A., et. al.: Navigation with electromagnetic tracking for interventional radiology procedures: a feasibility study. J Vasc Interv Radiol 2005; 16: pp. 493-505.
26. Markert M., Koschany A., Lueth T.: Tracking of the liver for navigation in open surgery. Int J Comput Assist Radiol Surg 2010; 5: pp. 229-235.
27. Maier-Hein L., Maleike D., Neuhaus J., et. al.: Soft tissue navigation using needle-shaped markers: evaluation of navigation aid tracking accuracy and CT registration. Proc SPIE Med Imaging 2007; 6509: pp. 650926.
28. Silverman S.G., Deuson T.E., Kane N., et. al.: Percutaneous abdominal biopsy: cost-identification analysis. Radiology 1998; 206: pp. 429-435.
29. McGill D.B., Rakela J., Zinsmeister A.R., et. al.: A 21-year experience with major hemorrhage after percutaneous liver biopsy. Gastroenterology 1990; 99: pp. 1396-1400.
30. Janes C.H., Lindor K.D.: Outcome of patients hospitalized for complications after outpatient liver biopsy. Ann Intern Med 1993; 118: pp. 96-98.
31. Stattaus J., Kuehl H., Ladd S., et. al.: CT-guided biopsy of small liver lesions: visibility, artifacts, and corresponding diagnostic accuracy. Cardiovasc Intervent Radiol 2007; 30: pp. 928-935.
32. Haage P., Piroth W., Staatz G., et. al.: CT-guided percutaneous biopsies for the classification of focal liver lesions: a comparison between 14 G and 18 G puncture biopsy needles. Rofo 1999; 171: pp. 44-48.
33. Stattaus J., Kühl H., Hauth E.A., et. al.: Liver biopsy under guidance of multislice computed tomography: comparison of 16G and 18G biopsy needles. Radiologe 2007; 47: pp. 430-438.
34. Piccinino F., Sagnelli E., Pasquale G., et. al.: Complications following percutaneous liver biopsy. A multicenter retrospective study on 68,276 biopsies. J Hepatol 1986; 2: pp. 165-173.
35. Cadranel J.F., Rufat P., Degos F.: Group of Epidemiology of the French Association for the Study of the Liver (AFEF). Practices of liver biopsy in France: results of a prospective nationwide study. Hepatology 2000; 32: pp. 477-481.