
Rationale and Objectives
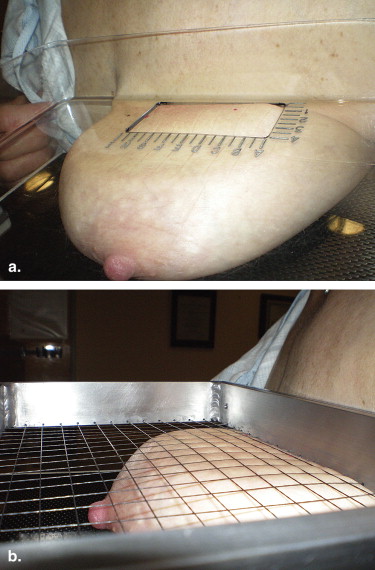
Current wire localization compression paddles provide a limited access window with no compression in this window. We describe a new compression paddle that addresses these issues and report on preliminary patient testing.
Materials and Methods
Four mechanical engineering students collaborated with a medical physicist, a radiographer, and two radiologists. Several concept designs were developed, one of which used a mesh surface. This went on to prototype development. After phantom testing, internal review board approval, US Food and Drug Administration waiver for nonsignificant risk device, and Medicare Part A exemption were obtained, the device was used in 10 patients going to wire localization for medical indications. Informed consent was obtained and a range of breast size was included. Wires were positioned from superior, lateral, and medial approach.
Results
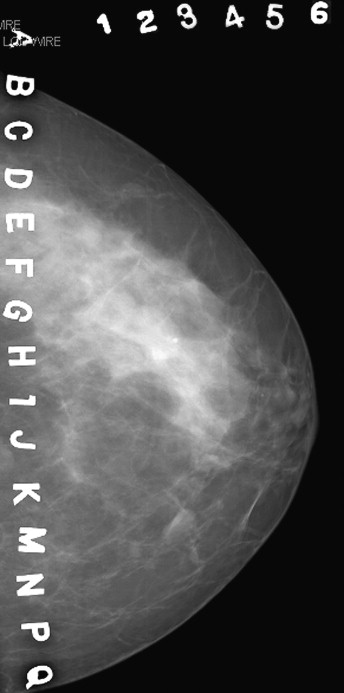
A total of 10 wires were successfully positioned in nine patients. The one technical failure was due to inadequate access to the axillary region because of the single prototype size. The grid system provided accurate localization of suspicious findings. The mesh was not visible in digital mammograms so there was no interference.
Conclusion
The new paddle improves on currently available models. Advantages included lack of visual (on imaging) and technical interference from the compression mesh, and compression of the active window allowed localization of subtle findings. The large active area facilitated multiple wire placements within a single window. All localizations were easily performed on the initial image because of the large active window, obviating the need for acquisition of additional images and the associated additional radiation.
Wire localization for surgical excision of a mammographic finding has changed with the advent of stereotactic vacuum-assisted and ultrasound-guided core biopsy. The cases referred for wire localization now seem to fall into three distinct categories. The first are those with a prior core biopsy and a microclip marking the area to be localized . These small metallic marker clips greatly facilitate the procedure. The second category cannot be localized for core biopsy because of location and or subtlety of the calcifications, mass or, asymmetry . These difficult cases seem to be increasing as a result of the improved image quality afforded by the newer digital units with a concomitant earlier identification of suspicious findings. The suspicious findings in such cases are often difficult to image without good compression and occasionally magnification. The third group of wire localization cases consists of those requiring bracketing wires in an attempt to conservatively manage the patient with lumpectomy instead of mastectomy . Placement of a second or third wire is not always possible with the initial small window used for localization of the first wire. This results in additional acquisition of images for each additional wire.
Current wire localization compression paddles provide a limited access window with no compression in this window. At our university, mechanical engineering students must complete a senior year design and manufacturing project. Projects are solicited from industry and the university at large. We submitted the development of a new wire localization compression paddle to overcome current design flaws as a potential project. The project was accepted. In this paper, we describe a new compression paddle that addresses our issues and report on preliminary patient testing.
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Patient Information
Patient Age Number Wires Indication Approach Results 1 49 1 Right suspicious calcifications
Left lumpectomy DCIS Superior Benign
Fibrocystic 2 42 1 Core BX complex fibroadenoma Superior Fibroadenoma 3 47 1 Suspicious mass at biopsy site of prior phyllodes tumor Medial Benign Phyllodes 4 45 1 Atypia on core BX
Wire microclip Superior Atypia 5 48 1 Suspicious calcifications
Failed attempted core BX Axillary
Failed Sclerosing adenosis 6 44 2 FNA × 2 nondiagnostic Superior Fibrocystic 7 75 1 Invasive ductal carcinoma
BX left microclip Superior IDC 8 54 1 Suspicious calcifications Lateral Fibroadenoma 9 56 1 Invasive ductal carcinoma Core BX microclip Medial IDC 10 75 1 Mass in duct on US Lateral Papilloma
BX, biopsy; DCIS, ductal carcinoma in situ; FNA, fine-needle biopsy; IDC, invasive ductal cancer; US, ultrasound.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Rosen E.L., Vo T.T.: Metallic clip deployment during stereotactic breast biopsy: retrospective analysis. Radiology 2001; 218: pp. 510-516.
2. Kopans D.B.: Preoperative imaging guided needle placement and localization of clinically occult lesions. In: Breast Imaging.1989.JB LippincottPhiladelphia, PA
3. Kirstein L.J., Rafferty E., Specht M.C., et. al.: Outcomes of multiple wire localization for larger breast cancers: when can mastectomy be avoided?. Am Coll Surg 2008; 207: pp. 342-346.
4. Burkholder H.C., Witherspoon L.E., Burns R.P., et. al.: Breast surgery techniques: preoperative bracketing wire localization by surgeons. Am Surg 2007; 73: pp. 574-578.
5. Liberman L., Kaplan J., Van Zee K.J., et. al.: Bracketing wires for preoperative breast needle localization. AJR Am J Roentgenol 2001; 177: pp. 565-572.
6. MQSA standards. Available at: http://www.fda.gov/Radiation-EmittingProducts/MammographyQualityStandardsActandProgram/Guidance/PolicyGuidanceHelpSystem/ucm053604.htm . Accessed October 2, 2009.
7. Booi R.C., Krücker J.F., Goodsitt M.M., et. al.: Evaluating thin compression paddles for mammographically compatible ultrasound. Ultrasound Med Biol 2007; 33: pp. 472-482.