
Rationale and Objectives
The aims of this study were to evaluate high spectral and spatial resolution (HiSS) magnetic resonance imaging (MRI) for the diagnosis of breast cancer without the injection of contrast media by comparing the performance of precontrast HiSS images to that of conventional contrast-enhanced, fat-suppressed, T1-weighted images on the basis of image quality and in the task of classifying benign and malignant breast lesions.
Materials and Methods
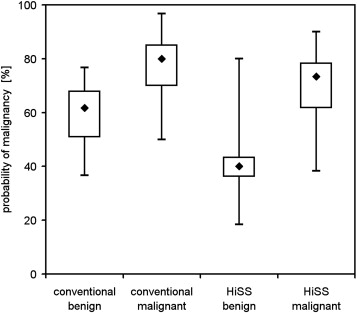
Ten benign and 44 malignant lesions were imaged at 1.5 T with HiSS (precontrast administration) and conventional fat-suppressed imaging (3–10 minutes after contrast administration). This set of 108 images, after randomization, was evaluated by three experienced radiologists blinded to the imaging technique. Breast Imaging Reporting and Data System morphologic criteria (lesion shape, lesion margin, and internal signal intensity pattern) and final assessment were used to measure reader performance. Image quality was evaluated on the basis of boundary delineation and quality of fat suppression. An overall probability of malignancy was assigned to each lesion for HiSS and conventional images separately.
Results
On boundary delineation and quality of fat suppression, precontrast HiSS scored similarly to conventional postcontrast MRI. On benign versus malignant lesion separation, there was no statistically significant difference in receiver-operating characteristic performance between HiSS and conventional MRI, and HiSS met a reasonable noninferiority condition.
Conclusions
Precontrast HiSS imaging is a promising approach for showing lesion morphology without blooming and other artifacts caused by contrast agents. HiSS images could be used to guide subsequent dynamic contrast-enhanced MRI scans to maximize spatial and temporal resolution in suspicious regions. HiSS MRI without contrast agent injection may be particularly important for patients at risk for contrast-induced nephrogenic systemic fibrosis or allergic reactions.
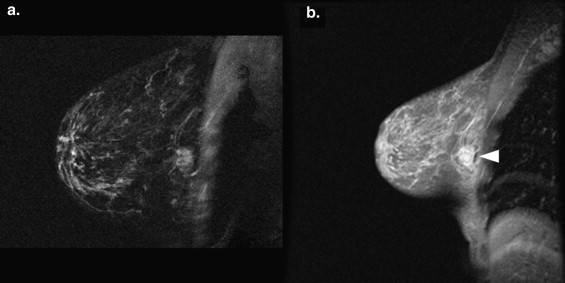
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI), combined with high-resolution postcontrast anatomic imaging, is an important tool for the routine clinical detection and diagnosis of breast cancer . However, although its sensitivity is reported as consistently high (75%–100%), its specificity has been variable (29%–90%) . A number of factors can reduce the utility of DCE-MRI in assessing lesion morphology: the magnetic susceptibility of contrast agents, as well as contrast agent diffusion and/or convection, causes increased blurring at tissue boundaries . Rapid changes in contrast media concentration during image acquisition can change lesion contrast and thus contribute additional blurring in the phase-encoding direction. These effects can obscure the lesion margin and make morphologic assessment more difficult (see Fig 1 ). In addition, contrast agent administration is contraindicated in a small but significant percentage of the population because of the risk for contrast agent–induced nephrogenic systemic fibrosis or allergic reactions . These issues could be addressed by effective imaging without contrast agents.
 Open full size image
Open full size image
Figure 1
A 69-year-old woman with an invasive ductal carcinoma lesion was imaged using high spectral and spatial resolution (HiSS) and conventional imaging. (a) HiSS water peak height (repetition time, 500 ms; echo time, 90 ms; in-plane resolution, 1 mm) and (b) conventional T1-weighted (repetition time, 12.6 ms; echo time, 3.8 ms; in-plane resolution, 1 mm) sagittal images are shown. The lesion is indicated with an arrow . Spiculations surrounding the lesion are much better visualized in the HiSS image, probably because of contrast agent diffusion from the lesion in the dynamic contrast-enhanced magnetic resonance image.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
MRI Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
High Spectral and Spatial Resolution Imaging Sequence Parameters
Parameter Philips Achieva ∗ GE Signa † Repetition time (ms) 500 250–500 Effective echo time (ms) 90 96–192 Flip angle (°) 90 60 Echo train length 128 64–128 Echo spacing (ms) 1.4 3 Spectral bandwidth (Hz) 715 333 Spectral resolution (Hz) 5.6 2.6–5.2 Field of view, readout direction (mm) 256 240–360 Field of view, phase encode direction (mm) 256 120–180 Acquisition matrix 256 × 256 384 × 192 In-plane resolution (mm) 1 0.65–0.95 Slice thickness (mm) 3 3–4 Number of slices imaged 1 1–2 Acquisition time 2 min 8 s 1 min 36 s
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
HiSS Data Processing
Get Radiology Tree app to read full this article<
Radiologist Evaluation
Get Radiology Tree app to read full this article<
Table 2
BI-RADS Assessment Categories Used
BI-RADS Category Values Lesion shape Round, oval, lobular, irregular Lesion margin Smooth, irregular, spiculated Internal signal intensity pattern Homogeneous, heterogeneous, dark internal septations, bright internal septations, rim (peripheral hyperintensity), central hyperintensity Final BI-RADS assessment 0–5
BI-RADS, Breast Imaging Reporting and Data System.
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Overall
Get Radiology Tree app to read full this article<
BI-RADS Measures
Get Radiology Tree app to read full this article<
Image Quality Measures
Get Radiology Tree app to read full this article<
Probability of Malignancy Measure
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
![Figure 5, Receiver-operating characteristic plots with probability of malignancy as a classifier, and proper binormal model fits to the data, are shown for conventional T1-weighted ( solid circles, dotted line ) and high spectral and spatial resolution (HiSS) ( open circles, solid line ) images. The areas under the curves for conventional and HiSS images are 0.81 and 0.84, respectively (difference, 0.036; 95% confidence interval [CI], −0.25 to 0.32), for reader A; 0.86 and 0.83 (difference, −0.028; 95% CI, −0.26, 0.20) for reader B; and 0.76 and 0.91 (difference, 0.16; 95% CI, 0.02 to 0.30) for reader C. There is no statistically significant difference in the overall performance of the two imaging methods.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/NoncontrastEnhancedMRIforEvaluationofBreastLesions/3_1s20S1076633211003928.jpg)
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Saslow D., Boetes C., Burke W., et. al.: American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin 2007; 57: pp. 75-89.
2. Swayampakula A.K., Dillis C., Abraham J.: Role of MRI in screening, diagnosis and management of breast cancer. Exp Rev Anticancer Ther 2008; 8: pp. 811-817.
3. Warner E., Messersmith H., Causer P., et. al.: Systematic review: using magnetic resonance imaging to screen women at high risk for breast cancer. Ann Intern Med 2008; 148: pp. 671-679.
4. Kuhl C.K., Mielcareck P., Klaschik S., et. al.: Dynamic breast MR imaging: are signal intensity time course data useful for differential diagnosis of enhancing lesions?. Radiology 1999; 211: pp. 101-110.
5. Huang W., Fisher P.R., Dulaimy K., et. al.: Detection of breast malignancy: diagnostic MR protocol for improved specificity. Radiology 2004; 232: pp. 585-591.
6. Bluemke D.A., Gatsonis C.A., Chen M.H., et. al.: Magnetic resonance imaging of the breast prior to biopsy. JAMA 2004; 292: pp. 2735-2742.
7. Kuhl C.K., Schild H.H., Morakkabati N.: Dynamic bilateral contrast-enhanced MR imaging of the breast: trade-off between spatial and temporal resolution. Radiology 2005; 236: pp. 789-800.
8. Kneeshaw P.J., Lowry M., Manton D., et. al.: Differentiation of benign from malignant breast disease associated with screening detected microcalcifications using dynamic contrast enhanced magnetic resonance imaging. Breast 2006; 15: pp. 29-38.
9. Penn A., Thompson S., Brem R., et. al.: Morphologic blooming in breast MRI as a characterization of margin for discriminating benign from malignant lesions. Acad Radiol 2006; 13: pp. 1344-1354.
10. Perazella M.A.: Gadolinium-contrast toxicity in patients with kidney disease: nephrotoxicity and nephrogenic systemic fibrosis. Curr Drug Safety 2008; 3: pp. 67-75.
11. Fan X., Abe H., Medved M., et. al.: Fat suppression with spectrally selective inversion vs. high spectral and spatial resolution MRI of breast lesions: qualitative and quantitative comparisons. J Magn Reson Imaging 2006; 24: pp. 1311-1315.
12. Medved M., Newstead G.M., Abe H., et. al.: High spectral and spatial resolution MRI of breast lesions: preliminary clinical experience. AJR Am J Roentgenol 2006; 186: pp. 30-37.
13. Karczmar G.S., Du W., Medved M., et. al.: Spectrally inhomogeneous effects of contrast agents in breast lesion detected by high spectral and spatial resolution MRI. Acad Radiol 2002; 9: pp. S352-S354.
14. Foxley S., Fan X., Mustafi D., et. al.: Sensitivity to tumor microvasculature without contrast agents in high spectral and spatial resolution MR images. Magn Reson Med 2009; 61: pp. 291-298.
15. Harms S.E., Flamig D.P., Hesley K.L., et. al.: Fat-suppressed three-dimensional MR imaging of the breast. Radiographics 1993; 13: pp. 247-267.
16. Soderstrom C.E., Harms S.E., Copit D.S., et. al.: Three-dimensional RODEO breast MR imaging of lesions containing ductal carcinoma in situ. Radiology 1996; 201: pp. 427-432.
17. Du W., Du Y.P., Bick U., et. al.: Breast MR imaging with high spectral and spatial resolutions: preliminary experience. Radiology 2002; 224: pp. 577-585.
18. Medved M., Du W., Zamora M.A., et. al.: The effect of varying spectral resolution on the quality of high spectral and spatial resolution magnetic resonance images of the breast. J Magn Reson Imaging 2003; 18: pp. 442-448.
19. Medved M., Newstead G.M., Fan X., et. al.: Fourier component imaging of water resonance in the human breast provides markers for malignancy. Phys Med Biol 2009; 54: pp. 5767-5779.
20. Medved M., Newstead G.M., Fan X., et. al.: Fourier components of inhomogeneously broadened water resonances in breast: a new source of MRI contrast. Magn Reson Med 2004; 52: pp. 193-196.
21. Pinker K., Grabner G., Bogner W., et. al.: A combined high temporal and high spatial resolution 3 Tesla MR imaging protocol for the assessment of breast lesions: initial results. Invest Radiol 2009; 44: pp. 553-558.
22. Jansen S.A., Fan X., Medved M., et. al.: Characterizing early contrast uptake of ductal carcinoma in situ with high temporal resolution dynamic contrast-enhanced MRI of the breast: a pilot study. Phys Med Biol 2010; 55: pp. N473-N485.
23. Medved M., Newstead G.M., Abe H., et. al.: Clinical implementation of a multislice high spectral and spatial resolution-based MRI sequence to achieve unilateral full-breast coverage. Magn Reson Imaging 2010; 28: pp. 16-21.
24. Medved M., Ivancevic M.K., Olopade O.I., et. al.: Echo-planar spectroscopic imaging (EPSI) of the water resonance structure in human breast using sensitivity encoding (SENSE). Magn Reson Med 2010; 63: pp. 1557-1563.
25. Doyle M., Mansfield P.: Chemical-shift imaging: a hybrid approach. Magn Reson Med 1987; 5: pp. 255-261.
26. Mansfield P.: Spatial mapping of the chemical shift in NMR. Magn Reson Med 1984; 1: pp. 370-386.
27. Dorfman D.D., Berbaum K.S., Metz C.E.: Receiver operating characteristic rating analysis. Generalization to the population of readers and patients with the jackknife method. Invest Radiol 1992; 27: pp. 723-731.
28. Dorfman D.D., Berbaum K.S., Lenth R.V., et. al.: Monte Carlo validation of a multireader method for receiver operating characteristic discrete rating data: factorial experimental design. Acad Radiol 1998; 5: pp. 591-602.
29. Hillis S.L., Berbaum K.S.: Power estimation for the Dorfman-Berbaum-Metz method. Acad Radiol 2004; 11: pp. 1260-1273.
30. Hillis S.L., Berbaum K.S.: Monte Carlo validation of the Dorfman-Berbaum-Metz method using normalized pseudovalues and less data-based model simplification. Acad Radiol 2005; 12: pp. 1534-1541.
31. Hillis S.L., Obuchowski N.A., Schartz K.M., et. al.: A comparison of the Dorfman-Berbaum-Metz and Obuchowski-Rockette methods for receiver operating characteristic (ROC) data. Stat Med 2005; 24: pp. 1579-1607.
32. Hillis S.L.: A comparison of denominator degrees of freedom methods for multiple observer ROC analysis. Stat Med 2007; 26: pp. 596-619.
33. Hillis S.L., Berbaum K.S., Metz C.E.: Recent developments in the Dorfman-Berbaum-Metz procedure for multireader ROC study analysis. Acad Radiol 2008; 15: pp. 647-661.
34. Pesce L.L., Metz C.E.: Reliable and computationally efficient maximum-likelihood estimation of “proper” binormal ROC curves. Acad Radiol 2007; 14: pp. 814-829.
35. Harms S.E., Flamig D.P., Hesley K.L., et. al.: MR imaging of the breast with rotating delivery of excitation off resonance: clinical experience with pathologic correlation. Radiology 1993; 187: pp. 493-501.
36. Soderstrom C.E., Harms S.E., Farrell R.S., et. al.: Detection with MR imaging of residual tumor in the breast soon after surgery. AJR Am J Roentgenol 1997; 168: pp. 485-488.