
Rationale and Objectives
Evidence-based treatment and management for patients with bronchiectasis remain challenging. There is a need for regional disease measurements as focal distribution of disease is common. Our objective was to evaluate the ability of magnetic resonance imaging (MRI) to detect regional ventilation impairment and response to airway clearance therapy (ACT) in patients with noncystic fibrosis (CF) bronchiectasis, providing a new way to objectively and regionally evaluate response to therapy.
Materials and Methods
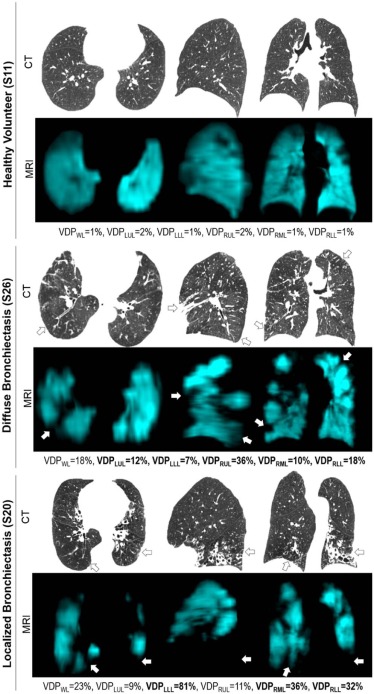
Fifteen participants with non-CF bronchiectasis and 15 age-matched healthy volunteers provided written informed consent to an ethics board-approved Health Insurance Portability and Accountability Act-compliant protocol and underwent spirometry, plethysmography, computed tomography (CT), and hyperpolarized 3 He MRI. Bronchiectasis patients also completed a Six-Minute Walk Test, the St. George’s Respiratory questionnaire, and Patient Evaluation Questionnaire (PEQ), and returned for a follow-up visit after 3 weeks of daily oscillatory positive expiratory pressure use. CT evidence of bronchiectasis was qualitatively reported by lobe, and MRI ventilation defect percent (VDP) was measured for the entire lung and individual lobes.
Results
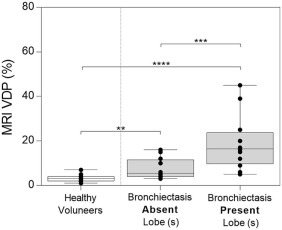
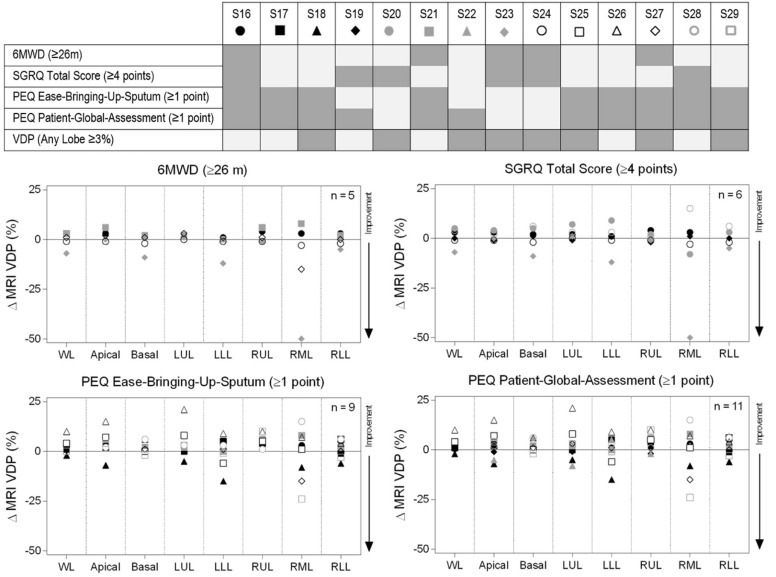
CT evidence of bronchiectasis and abnormal VDP (14 ± 7%) was observed for all bronchiectasis patients and no healthy volunteers. There was CT evidence of bronchiectasis in all lobes for 3 patients and in 3 ± 1 lobes (range = 1–4) for 12 patients. VDP in lobes with CT evidence of bronchiectasis (19 ± 12%) was significantly higher than in lobes without CT evidence of bronchiectasis (8 ± 5%, P = .001). For patients, VDP in lung lobes with ( P < .0001) and without CT evidence of bronchiectasis ( P = .006) was higher than in healthy volunteers (3 ± 1%). For all patients, mean PEQ-ease-bringing-up-sputum ( P = .048) and PEQ-patient-global-assessment ( P = .01) were significantly improved post-oscillatory positive expiratory pressure. An improvement in regional VDP greater than the minimum clinical important difference was observed for 8 of the 14 patients evaluated.
Conclusions
There was CT and MRI evidence of structure-function abnormalities in patients with bronchiectasis; in approximately half, there was evidence of ventilation improvements after airway clearance therapy.
Introduction
Bronchiectasis, a chronic airway disease, is characterized by irreversible dilation of the airways leading to pooling and poor clearance of mucus in affected regions . There is considerable overlap betweenbronchiectasis and other chronic airway diseases such as cystic fibrosis (CF) and chronic obstructive pulmonary disease (COPD). In fact, up to 50% of patients with COPD have associated bronchiectasis and these patients have higher rates of exacerbation and worse outcomes . The increasing prevalence and clinical impact of bronchiectasis are now recognized due to their significant burden on patients of all ages and on global healthcare costs.
Evidence-based treatment and management for patients with bronchiectasis remain very challenging. The overall goal of treatment is to improve quality of life by reducing cough, sputum volume, sputum purulence, and the number of chest infections. Unfortunately, despite the increasing number of randomized controlled trials in recent years, currently there are no pharmacological treatments approved, and clinical trials struggle to achieve enrollment targets and demonstrate treatment effects . Despite these challenges, numerous antibiotics, mucoactive therapies, anti-inflammatory agents, and chest physiotherapy are currently under investigation . Regional disease measurements may be particularly important in bronchiectasis because focal distribution of disease is quite common. For example, idiopathic bronchiectasis often affects the lower lobes, immotile cilia syndrome has a right middle lobe, and lingula predominance and allergic bronchopulmonary aspergillosis typically present centrally . Because of this, evidence-based treatments for patients with bronchiectasis will become increasingly dependent on sensitive, objective, and regional markers of lung function in proof-of-concept trials.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Study Subjects and Design
Get Radiology Tree app to read full this article<
Pulmonary Function, 6MWT, and Questionnaires
Get Radiology Tree app to read full this article<
MRI and CT Acquisition Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MRI and CT Image Analysis
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Methods
Get Radiology Tree app to read full this article<
Results
Subject Characteristics
Get Radiology Tree app to read full this article<
Table 1
Baseline Demographic, and Clinical and MRI Measurements
Parameter
(±SD) Bronchiectasis
(n = 15) Age, years 69(10) Male/Female 4/11 BMI, kg/m 2 24(4) FEV 1 % pred 69(21) FVC % pred 74(20) FEV 1 /FVC % 71(10) RV % pred 129(32) TLC % pred 97(16) RV/TLC % pred 133(25) DL CO % pred 65(20) 6MWD m 420(84) SGRQ total score 45(18)PEQ Cough frequency 3.6(1.0) Ease-bringing-up-sputum 4.0(0.4) Patient-global-assessment 4.0(0.4)MRI VDP WL % 14(7) VDP LUL % 9(5) VDP LLL % 20(19) VDP RUL % 13(9) VDP RML % 24(21) VDP RLL % 19(15)
BMI, body mass index; DL CO, carbon monoxide diffusion capacity of the lung; FEV 1, forced expiratory volume in 1 second; FVC, Forced vital capacity; LLL, left lower lobe; LUL, left upper lobe; MRI, magnetic resonance imaging; PEQ, Patient Evaluation Questionnaire; RLL, right lower lobe; RML, right middle lobe; RUL, right upper lobe; RV, residual volume; SD, standard deviation; SGRQ, St. George’s Respiratory Questionnaire; TLC, total lung capacity; VDP, ventilation defect percent; WL, whole lung; 6MWD, Six-Minute Walk Distance; % pred, percent predicted.
Get Radiology Tree app to read full this article<
CT and MRI Evidence of Bronchiectasis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Post-oPEP Treatment Measurements
Get Radiology Tree app to read full this article<
Table 2
Pre- and Post-oPEP Measurements
Parameter
(±SD) Pre-oPEP
(n = 14) Post-oPEP
(n = 14) Significance of Difference
(corrected P ) \* FEV 1 % pred 69(22) 68(22) .96 FVC % pred 74(21) 75(20) 1.00 6MWD m 419(87) 435(82) .27 SGRQ Total Score 42(15) 41(15) 1.00PEQ Cough frequency 3.6(1.0) 2.9(0.8) .09 Ease-Bringing-Up-Sputum 4.0(0.4) 2.9(1.0).048 Patient-Global-Assessment 4.0(0.4) 2.6(1.1).01MRI VDP WL % 15(7) 17(9) .78 VDP LUL % 9(5) 12(8) 1.00 VDP LLL % 21(20) 21(21) .72 VDP RUL % 13(9) 16(12) .20 VDP RML % 25(21) 20(15) 1.00 VDP RLL % 20(15) 21(16) 1.00
FEV 1, forced expiratory volume in 1 second; FVC, forced vital capacity; LLL, left lower lobe; LUL, left upper lobe; MRI, magnetic resonance imaging; PEQ, Patient Evaluation Questionnaire; RLL, right lower lobe; RML, right middle lobe; RUL, right upper lobe; SD, standard deviation; SGRQ, St. George’s Respiratory Questionnaire; VDP, ventilation defect percent; WL, whole lung; 6MWD, Six-Minute Walk Distance; % pred, percent predicted.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Appendix
Supplementary Data
Get Radiology Tree app to read full this article<
Appendix S1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Pasteur M.C., Bilton D., Hill A.T., et. al.: British Thoracic Society guideline for non-CF bronchiectasis. Thorax 2010; 65: pp. 577.
2. O’Brien C., Guest P.J., Hill S.L., et. al.: Physiological and radiological characterisation of patients diagnosed with chronic obstructive pulmonary disease in primary care. Thorax 2000; 55: pp. 635-642.
3. Patel I.S., Vlahos I., Wilkinson T.M., et. al.: Bronchiectasis, exacerbation indices, and inflammation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2004; 170: pp. 400-407.
4. Bilton D., Loebinger M.R., Wilson R.: Non-cystic fibrosis bronchiectasis: an evidence-base for new therapies. Lancet Respir Med 2014; 2: pp. 958-960.
5. Chalmers J.D., Aliberti S., Blasi F.: Management of bronchiectasis in adults. Eur Respir J 2015; 45: pp. 1446-1462.
6. Sidhu M.K., Mandal P., Hill A.T.: Bronchiectasis: an update on current pharmacotherapy and future perspectives. Expert Opin Pharmacother 2014; 15: pp. 505-525.
7. Cantin L., Bankier A.A., Eisenberg R.L.: Bronchiectasis. AJR Am J Roentgenol 2009; 193: pp. W158-W171.
8. Coxson H.O., Leipsic J., Parraga G., et. al.: Using pulmonary imaging to move chronic obstructive pulmonary disease beyond FEV1. Am J Respir Crit Care Med 2014; 190: pp. 135-144.
9. Altes T., Johnson M., Miller G., et. al.: Hyperpolarized gas MRI of ivacaftor therapy in subjects with cystic fibrosis who have the G551D-CFTR mutation. J Cyst Fibros 2012; 11: pp. S67.
10. Svenningsen S., Paulin G.A., Sheikh K., et. al.: Oscillatory positive expiratory pressure in chronic obstructive pulmonary disease. COPD 2016; 13: pp. 66-74.
11. Kirby M., Mathew L., Heydarian M., et. al.: Chronic obstructive pulmonary disease: quantification of bronchodilator effects by using hyperpolarized 3 He MR imaging. Radiology 2011; 261: pp. 283-292.
12. Mathew L., Kirby M., Farquhar D., et. al.: Hyperpolarized 3He functional magnetic resonance imaging of bronchoscopic airway bypass in chronic obstructive pulmonary disease. Can Respir J 2012; 19: pp. 41-43.
13. Kruger S.J., Niles D.J., Dardzinski B., et. al.: Hyperpolarized Helium-3 MRI of exercise-induced bronchoconstriction during challenge and therapy. J Magn Reson Imaging 2014; 39: pp. 1230-1237.
14. Costella S., Kirby M., Maksym G.N., et. al.: Regional pulmonary response to a methacholine challenge using hyperpolarized 3 He magnetic resonance imaging. Respirology 2012; 17: pp. 1237-1246.
15. Jones P.W., Quirk F.H., Baveystock C.M.: The St George’s respiratory questionnaire. Respir Med 1991; 85: pp. 25-31. discussion 33-27
16. Enright P.L.: The six-minute walk test. Respir Care 2003; 48: pp. 783-785.
17. Petty T.L.: The National Mucolytic Study. Results of a randomized, double-blind, placebo-controlled study of iodinated glycerol in chronic obstructive bronchitis. Chest 1990; 97: pp. 75-83.
18. Miller M.R., Hankinson J., Brusasco V., et. al.: Standardisation of spirometry. Eur Respir J 2005; 26: pp. 319-338.
19. Parraga G., Ouriadov A., Evans A., et. al.: Hyperpolarized 3He ventilation defects and apparent diffusion coefficients in chronic obstructive pulmonary disease: preliminary results at 3.0 Tesla. Invest Radiol 2007; 42: pp. 384-391.
20. Kirby M., Owrangi A., Svenningsen S., et. al.: On the role of abnormal DLCO in ex-smokers without airflow limitation: symptoms, exercise capacity and hyperpolarised helium-3 MRI. Thorax 2013; 68: pp. 752-759.
21. Christner J.A., Braun N.N., Jacobsen M.C., et. al.: Size-specific dose estimates for adult patients at CT of the torso. Radiology 2012; 265: pp. 841-847.
22. Guo F., Svenningsen S., Bluemke E., et. al.: Automated pulmonary lobar ventilation measurements using volume-matched thoracic CT and MRI. Proc SPIE 2015; 9417: pp. 9.
23. Ourselin S., Roche A., Subsol G., et. al.: Reconstructing a 3D structure from serial histological sections. Image Vis Comput 2001; 19: pp. 25-31.
24. Rueckert D., Sonoda L.I., Hayes C., et. al.: Nonrigid registration using free-form deformations: application to breast MR images. IEEE Trans Med Imaging 1999; 18: pp. 712-721.
25. Kirby M., Heydarian M., Svenningsen S., et. al.: Hyperpolarized 3 He magnetic resonance functional imaging semiautomated segmentation. Acad Radiol 2012; 19: pp. 141-152.
26. Puhan M.A., Chandra D., Mosenifar Z., et. al.: The minimal important difference of exercise tests in severe COPD. Eur Respir J 2011; 37: pp. 784-790.
27. Jones P.W.: St. George’s respiratory questionnaire: MCID. COPD 2005; 2: pp. 75-79.
28. Eliasziw M., Young S.L., Woodbury M.G., et. al.: Statistical methodology for the concurrent assessment of interrater and intrarater reliability: using goniometric measurements as an example. Phys Ther 1994; 74: pp. 777-788.
29. Nicolini A., Cardini F., Landucci N., et. al.: Effectiveness of treatment with high-frequency chest wall oscillation in patients with bronchiectasis. BMC Pulm Med 2013; 13: pp. 21.
30. Murray M.P., Pentland J.L., Hill A.T.: A randomised crossover trial of chest physiotherapy in non-cystic fibrosis bronchiectasis. Eur Respir J 2009; 34: pp. 1086-1092.
31. Figueiredo P.H., Zin W.A., Guimaraes F.S.: Flutter valve improves respiratory mechanics and sputum production in patients with bronchiectasis. Physiother Res Int 2012; 17: pp. 12-20.
32. Guimaraes F.S., Moco V.J., Menezes S.L., et. al.: Effects of ELTGOL and Flutter VRP1(R) on the dynamic and static pulmonary volumes and on the secretion clearance of patients with bronchiectasis. Rev Bras Fisioter 2012; 16: pp. 108-113.
33. Herrero-Cortina B., Vilaro J., Marti D., et. al.: Short-term effects of three slow expiratory airway clearance techniques in patients with bronchiectasis: a randomised crossover trial. Physiotherapy 2015;
34. Failo R., Wielopolski P.A., Tiddens H.A., et. al.: Lung morphology assessment using MRI: a robust ultra-short TR/TE 2D steady state free precession sequence used in cystic fibrosis patients. Magn Reson Med 2009; 61: pp. 299-306.
35. Tepper L.A., Ciet P., Caudri D., et. al.: Validating chest MRI to detect and monitor cystic fibrosis lung disease in a pediatric cohort. Pediatr Pulmonol 2016; 51: pp. 34-41.
36. Puderbach M., Eichinger M., Gahr J., et. al.: Proton MRI appearance of cystic fibrosis: comparison to CT. Eur Radiol 2007; 17: pp. 716-724.
37. Kirby M., Svenningsen S., Owrangi A., et. al.: Hyperpolarized 3He and 129Xe MR imaging in healthy volunteers and patients with chronic obstructive pulmonary disease. Radiology 2012; 265: pp. 600-610.