
Rationale and Objectives
To describe a little-known therapy-related small-airway phenomenon presumably caused by mucosal irritation in patients undergoing allogeneic stem cell transplantation (allo-SCT).
Materials and Methods
Retrospective database search at our institution identified 739 hematologic patients who underwent chemotherapy + allo-SCT between September 2004 and March 2014. After infectious pulmonary complications were excluded, 75 patients (female = 24; male = 51; median age = 47 years) with signs of generalized bronchiolitis (GB) on chest high-resolution computed tomography were identified. Computed tomography (CT) was performed proximate to chemotherapy onset; 92% had follow-up CT (mean, 1.9 weeks). The presence of centrilobular nodules, bronchial wall thickening (BWT), tree-in-bud (distributed diffuse vs. focal), ground-glass opacity, airspace opacification, luminal impactions, and air trapping was correlated with occurrence and duration of oral mucositis and therapy characteristics. Intensity of tree-in-bud and centrilobular nodules was graded absent (grade = 0), moderate (grade = 1), or marked (grade = 2).
Results
Overall incidence of GB among allo-SCT patients was 10.14%. GB was diagnosed at the time point of transplantation with a mean duration of CT findings of 4 weeks (±2.7). Tree-in-bud (17% [grade 2] and 83% [grade 1]) and BWT were present in 100% of the patients. Centrilobular nodules diffusely distributed were found in 45.5% of patients (20% [grade 2], 24% [grade 1], and 56% [none]). Air trapping and mosaic pattern were found in 13% and 16% of the patients, respectively. Resolution of GB was spontaneous. GB and its severity correlated with the temporal course and grade of oral mucositis; frequency and degree were not significantly influenced by the chemotherapy regimen. The incidence of GB in high-resolution computed tomography was statistically and significantly higher in patients with oral mucositis ( P < 0.035).
Conclusions
GB is frequent during chemotherapy for allo-SCT and is characterized by an even distribution of tree-in-bud, BWT, centrilobular nodules, mild clinical symptoms, and spontaneous resolution.
Introduction
llogeneic stem cell transplantation (allo-SCT) is a potential curative therapy for many hematologic diseases. Recently, reduced intensity conditioning (RIC) regimens have been developed to allow allo-SCT even in elderly patients. Unfortunately, these therapies are frequently accompanied by both infectious and noninfectious complications affecting primarily the lungs. Severe pulmonary complications occur in 40–60% of patients undergoing allo-SCT, causing increased transplant-related deaths . Classically, these pulmonary complications are categorized early or late (before versus after day 100 post transplant) depending on time elapsed after SCT. Bacterial, viral, and fungal infections are among the most common “very early” posttransplant pulmonary complications occurring within 2 weeks after therapy onset because of maximal immunodeficiency (neutropenic phase). Pulmonary edema, diffuse alveolar hemorrhage, transfusion-related acute lung injury, veno-occlusive disease, and mucositis are also frequent and have been extensively analyzed in particular in the setting of allo-SCT , but some (e.g. engraftment syndrome) are joining hematopoietic regeneration and are also frequent in the setting of autologous SCT . Treatment strategy depends primarily on differentiation between infectious and noninfectious pulmonary complications based on clinical, laboratory, and imaging markers that help for more accurate classification of these disorders. In the setting of respiratory symptoms and imaging findings compatible with small-airway diseases on chest high-resolution computed tomography (HRCT), lower respiratory tract infection, mostly caused by respiratory viruses and less frequently by bacteria, must be suspected. However, knowledge of potential mimics is essential for accurate patient management. At this point, mucosal barrier injury (mucositis) represents a common complication and a potential differential diagnosis affecting patients receiving cytotoxic preparative chemotherapy regimens prior to allo-SCT . Whereas clinical manifestations of oral and gastrointestinal mucositis are well known, involvement of bronchial and bronchiolar mucosa is generally running on a mild clinical or even subclinical level and has been therefore paid less attention.
Based on a single-center long-year experience in dealing with imaging in patients undergoing allo-SCT, we decided to retrospectively analyze all patients developing pulmonary complications during neutropenia with the focus on generalized bronchiolitis (GB). Our purpose was to characterize it from a radiological–clinical point of view, differentiate it from other mimics, and describe its spontaneous course.
Materials and Methods
Patient Characteristics
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 1
Underlying Diseases of All Patients Undergoing Stem Cell Transplantation and Incidence of Generalized Bronchiolitis
Overall GB Incidence_n_ %n % %Total 739 100 75 100 10.14 AML 355 48.04 41 54.66 11.54 ALL 91 12.31 13 17.33 14.28 NHL 84 11.37 5 6.66 5.95 MDS 51 6.90 12 16.00 23.52 Multiple myeloma 36 4.87 — — — CML 28 3.79 1 1.33 3.57 MPS 23 3.11 — — — OMF 17 2.30 — — — CLL 16 2.17 1 1.33 6.25 Pure red cell aplasia 15 2.03 — — — Aplastic anemia 10 1.35 2 2.69 20.00 Hodgkin’s lymphoma 7 0.95 — — — Secondary MDS 5 0.68 — — — Systemic sclerosis 1 0.14 — — —
ALL, acute lymphoblastic leukemia; AML, acute myelogenous leukemia; CLL, chronic lymphocytic leukemia; CML, chronic myeloid leukemia; GB, generalized bronchiolitis; MDS, myelodysplastic syndrome; MPS, myeloproliferative syndrome; NHL, non-Hodgkin lymphoma; OMF, osteomyelofibrosis.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
High-resolution CT Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Standard of Reference
Get Radiology Tree app to read full this article<
Statistics
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 2
Major CT Imaging Findings
Tree-in-bud sign (%) 100 Grade 1 83 Grade 2 17 Bronchial wall thickening (%) 97 Nodules (%) 45.5 Grade 0 56.0 Grade 1 24.0 Grade 2 20.0 Mosaic pattern (%) 16.0 Air trapping (%) 13.3 Mucoid impaction (%) 5 Bronchiectasia (%) 0
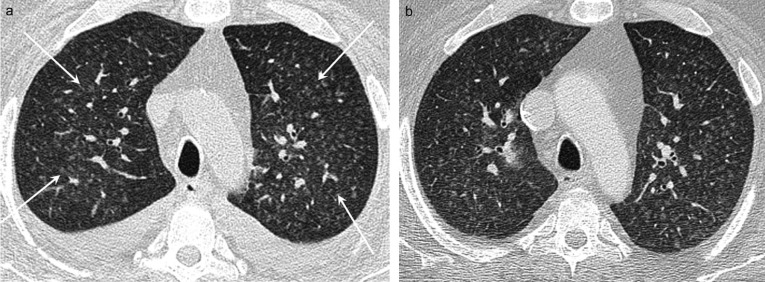
![Figure 1, (a–b) 55-year-old female patient with acute myeloid leukemia (AML). During chemotherapy with fludarabine and total body irradiation (TBI), the patient developed mild shortness of breath and subfebrile temperature. Chest CT performed at day 0 (same day as the stem cell transplantation–human leukocyte antigen [HLA] matched unrelated) revealed ubiquitous tree-in-bud, suggesting lower respiratory tract pathology ( a , white arrows ). Nasopharyngeal swab test was negative and neutrophils regenerated 3 weeks later. During the early posttransplantation phase, two repeat CTs were performed (at week 3 and 6) which showed first worsening of panbronchiolitis (not shown) and then rapid resolving of generalized bronchiolitis (GB) (b) . No antiviral therapy was instituted.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/NoninfectiousGeneralizedBronchiolitisintheSettingofAllogeneicStemCellTransplantation/0_1s20S1076633215003748.jpg)
![Figure 2, 39-year-old male patient with acute lymphocytic leukemia (ALL). The patient complained at day 0 after allo-SCT (human leukocyte antigen [HLA] identical sibling) of minimal symptoms of respiratory shortness and cough. He underwent chemotherapy with etoposide and TBI for conditioning and also received anti-thymocyte globulin (ATG). Chest CT performed at this time revealed an evenly distributed tree-in-bud sign ( white arrows ) suggestive of lower respiratory tract pathology. Tree-in-bud persisted for 6 weeks and then resolved entirely (not shown) without antiviral therapy. Nasopharyngeal swab test was negative for infection.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/NoninfectiousGeneralizedBronchiolitisintheSettingofAllogeneicStemCellTransplantation/1_1s20S1076633215003748.jpg)
![Figure 3, (a–b) 57-year-old female patient with myelodysplastic syndrome (MDS). She was conditioned with busulphan + fludarabine (FLAMSA protocol: fludarabine, cytarabine, and amsacrine). She also received anti-thymocyte globulin (ATG). At day 0 of allo-SCT (human leukocyte antigen [HLA] matched unrelated), the patient developed respiratory symptoms and neutropenic fever and therefore underwent chest CT. Besides pleural effusion on the left ( black asterisk ), grade II tree-in-bud combined with centrilobular nodular pattern was observed ( a , white arrows ). Two weeks later, GB resolved in part, whereas the pleural effusion proved progressive. All in all, the patient recovered in the next weeks without antiviral therapy.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/NoninfectiousGeneralizedBronchiolitisintheSettingofAllogeneicStemCellTransplantation/2_1s20S1076633215003748.jpg)
![Figure 5, 37-year-old female patient with myelodysplastic syndrome (MDS). The patient was conditioned with busulphan and cyclophosphamide. She also received anti-thymocyte globulin (ATG). Chest CT was performed at day 0 (allo-SCT–human leukocyte antigen [HLA] mismatch unrelated) because of a slight increase in C-reactive protein (CRP). Oral mucositis was diagnosed at the same time. Note the evenly distributed ill-defined centrilobular nodules that resolved in the next weeks without antiviral therapy.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/NoninfectiousGeneralizedBronchiolitisintheSettingofAllogeneicStemCellTransplantation/4_1s20S1076633215003748.jpg)
Get Radiology Tree app to read full this article<
The Course of Pulmonary Findings at Chest HRCT at Follow-up
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Correlation of Chest HRCT Imaging Findings and Their Incidence with the Chemotherapy Regimen, TBI, and Graft Characteristics
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 3
Elements of Conditioning Regimen
TBI ( n ) 35 Chemotherapy ( n ) Cyclophosphamide 29 Fludarabine 30 Busulfan 20 Melphalan 8 FLAMSA 7 Alternative idarubicin 2
FLAMSA, fludarabine, cytarabine, and amsacrine; TBI, total body irradiation.
Some patients received chemotherapy regimens consisting of a combination of more agents.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Comparing Patients’ Characteristics in the Group Developing GB Versus the Group with Allo-SCT without GB
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Krowka M.J., Rosenow E.C., Hoagland H.C.: Pulmonary complications of bone marrow transplantation. Chest 1985; 87: pp. 237-246.
2. Song I., Yi C.A., Han J., et. al.: CT findings of late-onset noninfectious pulmonary complications in patients with pathologically proven graft-versus-host disease after allogeneic stem cell transplant. AJR Am J Roentgenol 2012; 199: pp. 581-587.
3. Agusti C., Ramirez J., Picado C., et. al.: Diffuse alveolar hemorrhage in allogeneic bone marrow transplantation. A postmortem study. Am J Respir Crit Care Med 1995; 151: pp. 1006-1010.
4. Gupta S., Jain A., Warneke C.L., et. al.: Outcome of alveolar hemorrhage in hematopoietic stem cell transplant recipients. Bone Marrow Transplant 2007; 40: pp. 71-78.
5. Bunte M.C., Patnaik M.M., Pritzker M.R., et. al.: Pulmonary veno-occlusive disease following hematopoietic stem cell transplantation: a rare model of endothelial dysfunction. Bone Marrow Transplant 2008; 41: pp. 677-686.
6. Silliman C.C., Ambruso D.R., Boshkov L.K.: Transfusion-related acute lung injury. Blood 2005; 105: pp. 2266-2273.
7. Wallis J.P.: Transfusion-related acute lung injury (TRALI)—under-diagnosed and under-reported. Br J Anaesth 2003; 90: pp. 573-576.
8. Akasheh M., Eastwood D., Vesole D.H.: Engraftment syndrome after autologous hematopoietic stem cell transplant supported by granulocyte-colony-stimulating factor (G-CSF) versus granulocyte-macrophage colony-stimulating factor (GM-CSF). Bone Marrow Transplant 2003; 31: pp. 113-116.
9. Niscola P.: Mucositis in malignant hematology. Expert Rev Hematol 2010; 3: pp. 57-65.
10. Miller M.M., Donald D.V., Hagemann T.M.: Prevention and treatment of oral mucositis in children with cancer. J Pediatr Pharmacol Ther 2012; 17: pp. 340-350.
11. Hansell D.M., Bankier A.A., MacMahon H., et. al.: Fleischner Society: glossary of terms for thoracic imaging. Radiology 2008; 246: pp. 697-722.
12. Woo S.B., Sonis S.T., Monopoli M.M., et. al.: A longitudinal study of oral ulcerative mucositis in bone marrow transplant recipients. Cancer 1993; 72: pp. 1612-1617.
13. Peterson D.E., Bensadoun R.J., Roila F., et. al.: Management of oral and gastrointestinal mucositis: ESMO Clinical Practice Guidelines. Ann Oncol 2011; 22: pp. vi78-vi84.
14. Wardley A.M., Jayson G.C., Swindell R., et. al.: Prospective evaluation of oral mucositis in patients receiving myeloablative conditioning regimens and haemopoietic progenitor rescue. Br J Haematol 2000; 110: pp. 292-299.
15. McGuire D.B., Altomonte V., Peterson D.E., et. al.: Patterns of mucositis and pain in patients receiving preparative chemotherapy and bone marrow transplantation. Oncol Nurs Forum 1993; 20: pp. 1493-1502.
16. Gopal R., Ha C.S., Tucker S.L., et. al.: Comparison of two total body irradiation fractionation regimens with respect to acute and late pulmonary toxicity. Cancer 2001; 92: pp. 1949-1958.
17. Zerbe M.B., Parkerson S.G., Ortlieb M.L., et. al.: Relationships between oral mucositis and treatment variables in bone marrow transplant patients. Cancer Nurs 1992; 15: pp. 196-205.
18. Kremer J.M., Alarcon G.S., Weinblatt M.E., et. al.: Clinical, laboratory, radiographic, and histopathologic features of methotrexate-associated lung injury in patients with rheumatoid arthritis: a multicenter study with literature review. Arthritis Rheum 1997; 40: pp. 1829-1837.
19. Cameron I.L.: Cell renewal in the organs and tissues of the nongrowing adult mouse. Tex Rep Biol Med 1970; 28: pp. 203-248.
20. Ayers M.M., Jeffery P.K.: Proliferation and differentiation in mammalian airway epithelium. Eur Respir J 1988; 1: pp. 58-80.
21. Evans M.J., Cabral-Anderson L.J., Freeman G.: Effects of NO2 on the lungs of aging rats. II. Cell proliferation. Exp Mol Pathol 1977; 27: pp. 366-376.
22. Ryu J.H., Myers J.L., Swensen S.J.: Bronchiolar disorders. Am J Respir Crit Care Med 2003; 168: pp. 1277-1292.
23. Devakonda A., Raoof S., Sung A., et. al.: Bronchiolar disorders: a clinical-radiological diagnostic algorithm. Chest 2010; 137: pp. 938-951.
24. Gasparetto E.L., Escuissato D.L., Marchiori E., et. al.: High-resolution CT findings of respiratory syncytial virus pneumonia after bone marrow transplantation. AJR Am J Roentgenol 2004; 182: pp. 1133-1137.
25. Franquet T., Rodriguez S., Martino R., et. al.: Thin-section CT findings in hematopoietic stem cell transplantation recipients with respiratory virus pneumonia. AJR Am J Roentgenol 2006; 187: pp. 1085-1090.
26. Miller W.T., Barbosa E., Mickus T.J., et. al.: Chest computed tomographic imaging characteristics of viral acute lower respiratory tract illnesses: a case-control study. J Comput Assist Tomogr 2011; 35: pp. 524-530.
27. Miller W.T., Mickus T.J., Barbosa E., et. al.: CT of viral lower respiratory tract infections in adults: comparison among viral organisms and between viral and bacterial infections. AJR Am J Roentgenol 2011; 197: pp. 1088-1095.