
Rationale and Objectives
To determine the accuracy and sensitivity for dual-energy computed tomography (DECT) discrimination of uric acid (UA) stones from other (non-UA) renal stones in a commercially implemented product.
Materials and Methods
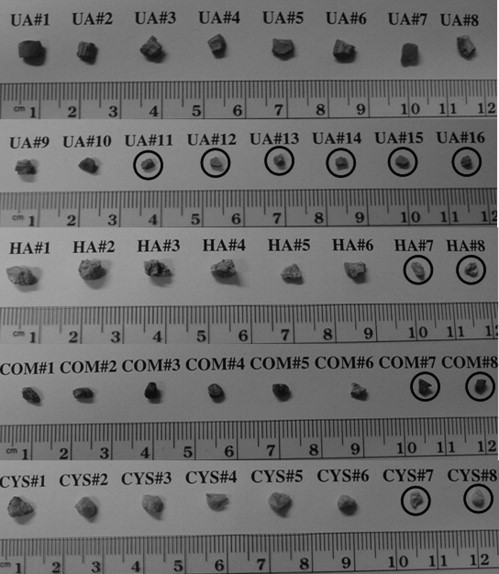
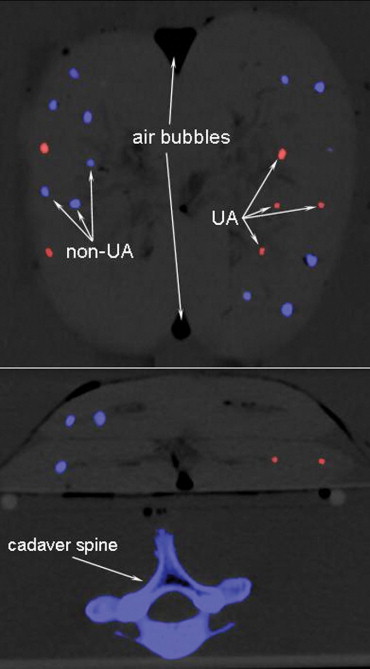
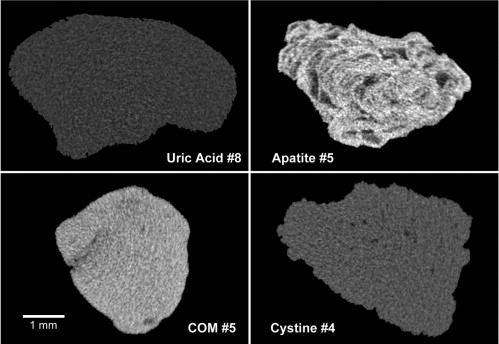
Forty human renal stones comprising uric acid ( n = 16), hydroxyapatite ( n = 8), calcium oxalate ( n = 8), and cystine ( n = 8) were inserted in four porcine kidneys (10 each) and placed inside a 32-cm water tank anterior to a cadaver spine. Spiral dual-energy scans were obtained on a dual-source, 64-slice computed tomography (CT) system using a clinical protocol and automatic exposure control. Scanning was performed at two different collimations (0.6 mm and 1.2 mm) and within three phantom sizes (medium, large, and extra large) resulting in a total of six image datasets. These datasets were analyzed using the dual-energy software tool available on the CT system for both accuracy (number of stones correctly classified as either UA or non-UA) and sensitivity (for UA stones). Stone characterization was correlated with micro-CT.
Results
For the medium and large phantom sizes, the DECT technique demonstrated 100% accuracy (40/40), regardless of collimation. For the extra large phantom size and the 0.6-mm collimation (resulting in the noisiest dataset), three (two cystine and one small UA) stones could not be classified (93% accuracy and 94% sensitivity). For the extra large phantom size and the 1.2-mm collimation, the dual-energy tool failed to identify two small UA stones (95% accuracy and 88% sensitivity).
Conclusions
In an anthropomorphic phantom model, dual-energy CT can accurately discriminate uric acid stones from other stone types.
Symptomatic urinary stone disease affects approximately 900,000 persons in the United States each year, resulting in annual medical cost of $5.3 billion. Nephrolithiasis has traditionally been evaluated using plain film radiographic techniques with or without tomography or administration of intravenous contrast for excretory urography. Over recent years, however, computed tomography (CT) has supplanted these traditional techniques because of increased sensitivity, speed, and the lack of intravenous contrast ( ). Furthermore, improved CT acquisition techniques can allow a lower radiation dose than was required for a traditional excretory urogram ( ).
Although state-of-the-art CT provides accurate submillimeter details of the size and location of renal stones ( ), current routine clinical image analysis does not differentiate stone composition. This is particularly important in the case of uric acid (UA) stones (∼10% of cases), because urinary alkalinization can be prescribed to dissolve UA stones and could thereby be initiated at presentation rather than following lengthy metabolic workup. Therefore simple and reliable differentiation of UA versus non-UA stone composition could potentially allow patients with UA stones to avoid invasive interventional urinary procedures for stone removal or external shock wave lithotripsy, both of which are expensive and might result in renal hemorrhage, fibrosis, or hypertension ( ).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
The Dose and Noise Levels for Different Phantom Sizes
Phantom Medium Size Large Size Extra Large Size Collimation 2 × 32 × 0.6 14 × 1.2 2 × 32 × 0.6 14 × 1.2 2 × 32 × 0.6 14 × 1.2 Dose (volume CT dose index) (mGy) 14.0 13.7 15.3 15.0 21.9 21.6 Noise (Hounsfield units) at 140 kVp 18 15 34 27 30 25 Noise (Hounsfield units) at 80 kVp 21 17 48 37 64 51
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 2
Accuracy and Sensitivity of Renal Stone Characterization with the New Dual-Energy Material Decomposition Algorithm
Experiment Accuracy ⁎ Sensitivity † All Stones Large Stones Small Stones ‡ All Stones Large Stones Small Stones ‡ Medium size 100% 100% 100% 100% 100% 100% Both collimations (40/40) (28/28) (12/12) (16/16) (10/10) (6/6) Large size 100% 100% 100% 100% 100% 100% Both collimations (40/40) (28/28) (12/12) (16/16) (10/10) (6/6) Extra large size 93% 93% 92% 94% 100% 83% 2 × 32 × 0.6 mm (37/40) (26/28) (11/12) (15/16) (10/10) (5/6) Extra large size 95% 100% 83% 88% 100% 67% 14 × 1.2 mm (38/40) (28/28) (10/12) (14/16) (10/10) (4/6)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Kawashima A., Vrtiska T.J., LeRoy A.J., et. al.: CT urography. Radiographics 2004; 24: pp. S35-S58.
2. Kalra M.K., Maher M.M., D’Souza R.V., et. al.: Detection of urinary tract stones at low-radiation-dose CT with z-axis automatic tube current modulation: phantom and clinical studies. Radiology 2005; 235: pp. 523-529.
3. Heneghan J.P., McGuire K.A., Leder R.A., et. al.: Helical CT for nephrolithiasis and ureterolithiasis: comparison of conventional and reduced radiation-dose techniques. Radiology 2003; 229: pp. 575-580.
4. Williams J.C., Kim S.C., Zarse C.A., et. al.: Progress in the use of helical CT for imaging urinary calculi. J Endourol 2004; 18: pp. 937-941.
5. Vrtiska T.J.: Quantitation of stone burden: imaging advances. Urol Res 2005; pp. 33398-33402.
6. Evan A.P., Willis L.R., Lingeman J.E., et. al.: Renal trauma and the risk of long-term complications in shock wave lithotripsy. Nephron 1998; 78: pp. 1-8.
7. Joseph P., Mandal A.K., Singh S.K., et. al.: Computerized tomography attenuation value of renal calculus: can it predict successful fragmentation of the calculus by extracorporeal shock wave lithotripsy?. J Urol 2002; 167: pp. 1968-1971.
8. Mostafavi M.R., Ernst R.D., Saltzman B.: Accurate determination of chemical composition of urinary calculi by spiral computerized tomography. J Urol 1998; 159: pp. 673-675.
9. Motley G., Dalrymple N., Keesling C., et. al.: Hounsfield unit density in the determination of urinary stone composition. Urology 2001; 58: pp. 170-173.
10. Nakada S.Y., Hoff D.G., Attai S., et. al.: Determination of stone composition by noncontrast spiral computed tomography in the clinical setting. Urology 2000; 55: pp. 816-819.
11. Pareek G., Armenakas N.A., Fracchia J.A.: Hounsfield units on computerized tomography predict stone-free rates after extracorporeal shock wave lithotripsy. J Urol 2003; 169: pp. 1679-1681.
12. Williams J.C., Paterson R.F., Kopecky K.K., et. al.: High resolution detection of internal structure of renal calculi by helical computerized tomography. J Urol 2002; 167: pp. 322-326.
13. Bellin M.F., Renard-Penna R., Conort P., et. al.: Helical CT evaluation of the chemical composition of urinary tract calculi with a discriminant analysis of CT-attenuation values and density. Eur Radiol 2004; 14: pp. 2134-2140.
14. Zarse C.A., McAteer J.A., Tann M., et. al.: Helical computed tomography accurately reports urinary stone composition using attenuation values: in vitro verification using high-resolution micro-computed tomography calibrated to fourier transform infrared microspectroscopy. Urology 2004; 63: pp. 828-833.
15. Mitcheson H.D., Zamenhof R.G., Bankoff M.S., et. al.: Determination of the chemical composition of urinary calculi by computerized tomography. J Urol 1983; 130: pp. 814-819.
16. Primak A.N., Fletcher J.G., Krauss B., et. al.: Non-invasive prediction of renal stone composition using high spatial resolution, dual-energy CT. Radiol Soc North Am Scient Assembly Annu Meeting 2006; pp. 753.
17. Zarse C.A., McAteer J.A., Sommer A.J., et. al.: Nondestructive analysis of urinary calculi using micro computed tomography. BMC Urol 2004; 4: pp. 15.
18. Daudon M., Donsimoni R., Hennequin C., et. al.: Sex- and age-related composition of 10 617 calculi analyzed by infrared spectroscopy. Urol Res 1995; 23: pp. 319-326.
19. Saw K.C., McAteer J.A., Monga A.G., et. al.: Helical CT of urinary calculi: effect of stone composition, stone size, and scan collimation. AJR Am J Roentgenol 2000; 175: pp. 329-332.
20. Williams J.C., Saw K.C., Monga A.G., et. al.: Correction of helical CT attenuation values with wide beam collimation: in vitro test with urinary calculi. Acad Radiol 2001; 8: pp. 478-483.