
Rationale and Objectives
To determine trends in nonvascular image-guided procedures at an urban general hospital over a 10-year period and to compare utilization of nonvascular interventional radiology (IR) over the decade 2001–2010 to a previously reported analysis for 1991–2000.
Methods
With institutional review board approval, a 20-year quality assurance database verified against the radiology information system was queried for procedure location (eg, pleura, liver, bowel, and abdomen) and type (eg, biopsy, catheter insertion, and transient drainage), demographics, and change over time. Yearly admissions and new hospital numbers assigned each year served to normalize for overall hospital activity.
Results
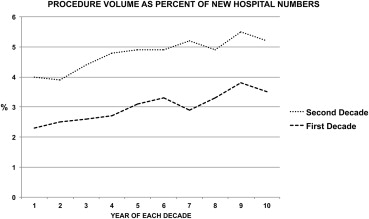
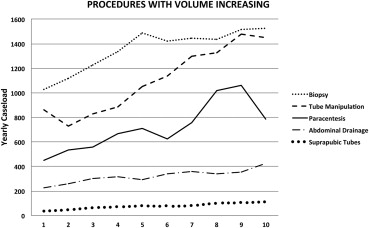
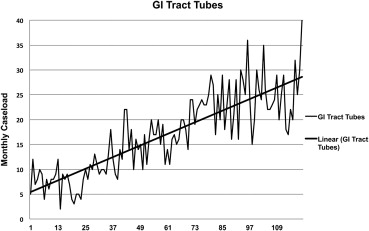
A total of 50,195 IR procedures were performed in 24,309 distinct patients (male:female, 12,625:11,684; average age, 60 years), 940 procedures performed in age <20 years, and 571 procedures performed in patients aged ≥90 years. A total of 15345, 4377, and 1754 patients had one, two, or three procedures, respectively; 470 had ≥10 procedures. Twenty-seven supervising radiologists and 277 individuals participated as operators, double the previous decade. Biopsy (4.8% average yearly increase), abdominal drainage (7.3%), paracentesis (12.9%), tube manipulation (13.0%), suprapubic bladder tube insertion (21.0%), and gastrostomy (44.6%) all increased strongly ( P < .001) over 120 months but not biliary drainage, nephrostomy, or chest tubes. Procedures increased faster than either admissions or new hospital numbers ( P < .001). For each 1000 new hospital numbers, IR service performed 48 procedures versus 31 the previous decade ( P < .0005).
Conclusions
Referrals for nonvascular IR procedures have doubled over 2 decades, outpacing growth in new hospital patients and requiring increased resource allocation.
Nonvascular interventional radiology (IR) includes an array of imaging-guided special procedures performed in organs and via access routes outside the vascular tree. So accepted and widespread are these techniques that it is impossible to imagine a modern hospital that cannot offer many of them to its patients. Such procedures are considered minimally invasive and include among many others percutaneous biopsy, abscess drainage, biliary, urinary, and gastrointestinal (GI) tract access, as well as simple fluid sampling or drainage like thoracentesis and paracentesis.
As a discipline, nonvascular IR has extensively evolved over the last 60 years. Percutaneous nephrostomy dates from 1955 . Biliary drainage evolved from purely diagnostic transhepatic cholangiography and angiography during the late 1970s . The details of percutaneous biopsy were worked out in the late 1970s and early 1980s by Haaga et al. and others . Gerzof et al. began to develop techniques for percutaneous abscess drainage around the same time. As Dondelinger has pointed out in his historical review of nonvascular IR, percutaneous abdominal abscess drainage has been recognized since the 1980s as a major advance for surgery . Techniques that permit a needle or small tube to accomplish what previously required surgery have been aided by improved imaging equipment such as real-time sonography and faster computed tomography (CT) scanners.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Average Weekday Staff Committed to Nonvascular IR, Based on Minimum Number of Procedures Performed
Fiscal Year ≥3 Procedures ≥8 Procedures 2001 1.74 0.78 2002 1.70 0.80 2003 1.91 0.83 2004 1.97 0.96 2005 2.16 1.07 2006 2.08 1.11 2007 2.32 1.18 2008 2.47 1.26 2009 2.54 1.43 2010 2.52 1.27
IR, interventional radiology.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Dunnick N.R., Illescas F.F., Mitchell S., et. al.: Interventional uroradiology. Invest Radiol 1989; 24: pp. 831-841.
2. Ferrucci J.T., Mueller P.R., Harbin W.P.: Percutaneous transhepatic biliary drainage: technique, results, and applications. Radiology 1980; 135: pp. 1-13.
3. Haaga J.R., Reich N.E., Havrilla T.R., et. al.: Computed tomography-guided biopsy. I. Overview. J Comput Tomogr 1978; 2: pp. 25-30.
4. Skolnick M.L., Dekker A., Weinstein B.J.: Ultrasound guided fine-needle aspiration biopsy of abdominal masses. Gastrointest Radiol 1978; 31: pp. 295-302.
5. Gerzof S.G., Robbins A.H., Birkett D.H.: Computed tomography in the diagnosis and management of abdominal abscesses. Gastrointest Radiol 1978; 31: pp. 287-294.
6. Dondelinger R.F.: A short history of non-vascular interventional radiology. J Belge Radiol 1995; 78: pp. 363-370.
7. Welch C.E., Malt R.A.: Abdominal surgery (third of three parts). N Engl J Med 1983; 308: pp. 753-760.
8. Hahn P.F., Gervais D.A., O’Neill M.J., et. al.: Nonvascular interventional procedures: analysis of a 10-year database containing more than 21,000 cases. Radiology 2001; 220: pp. 730-736.
9. Hahn P.F., Lee M.J., Gazelle G.S., et. al.: A simplified HyperCard data base for patient management in an interventional practice: experience with more than 4000 cases. AJR Am J Roentgenol 1994; 162: pp. 1443-1446.
10. Brown A.S., Mueller P.R., Ferrucci J.T.: Controlled percutaneous gastrostomy: nylon T-fastener for fixation of the anterior gastric wall. Radiology 1986; 158: pp. 543-545.
11. Riddell A.M., Charig M.J.: A survey of current practice in out of hours percutaneous nephrostomy insertion in the United Kingdom. Clin Radiology 2002; 57: pp. 1067-1069.
12. Hsia D., Musani A.I.: Interventional pulmonology. Med Clin North Am 2011; 95: pp. 1095-1114.
13. Nascimento R.G., Coleman J., Solomon S.B.: Current and future imaging for urologic interventions. Curr Opin Urol 2008; 18: pp. 116-121.
14. Foutch P.G., Haynes W.C., Bellapravalu S., et. al.: Percutaneous endoscopic gastrostomy (PEG). A new procedure comes of age. J Clin Gastrenterol 1986; 8: pp. 10-15.
15. Ginès P., Cárdenas A., Arroyo V., et. al.: Management of cirrhosis and ascites. N Engl J Med 2004; 350: pp. 1646-1654.
16. Nikolaidis P., vanSonnenberg E., Haddad Z.K., et. al.: Practice patterns of nonvascular interventional radiology procedures at academic centers in the United States?. Acad Radiol 2005; 12: pp. 1475-1482.