
Rationale and Objectives
This study aimed to determine if there were differences in the imaging features of normal lymph nodes between white and black women using magnetic resonance imaging.
Materials and Methods
Following institutional review board approval, we identified white and black women who underwent breast magnetic resonance imaging from November 1, 2008 to December 31, 2013 at our institution. To identify normal lymph nodes for measurement, patients with any benign or malignant causes for lymph node enlargement and patients with any subsequent breast cancer in the following 2 years were excluded. Black and white women were age matched at a 1:2 ratio. The largest lymph node in each axilla was measured for the long-axis length and maximal cortical thickness. Comparisons were made between white and black women using a conditional logistic regression to control for matching.
Results
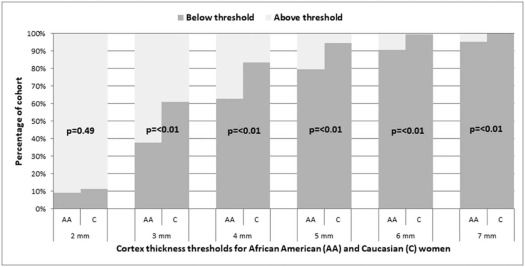
There were 55 black women and 110 white women for analysis. The mean lymph node long-axis length was 14.7 ± 5.3 mm for black women and 14.4 ± 6.4 mm for white women ( P = .678). The mean maximum cortical thickness was 3.3 ± 1.6 mm for black women and 2.6 ± 1.4 mm for Caucasian women ( P < .001). A significantly higher percentage of black than white women had cortical thicknesses greater than threshold values of 3, 4, 5, 6, and 7 mm ( P < .01 for all).
Conclusions
The normal lymph node cortical thickness in black women is significantly greater than in white women, which should be considered when deciding to recommend a lymph node biopsy.
Introduction
As part of the routine interpretation of breast magnetic resonance imaging (MRI), lymph node size and morphology in both axilla are assessed by the radiologist to determine if additional workup and possible biopsy should be recommended to assess for malignancy. This may occur in patients with known breast cancer for whom there has been regional metastatic spread, but abnormal lymph node morphology may be the presenting sign of a new otherwise unknown cancer from either the breast or another primary source . Although axillary lymph node biopsies are generally safe procedures, the proximity to major arteries and nerves increases the risk of complications compared to breast biopsies and thus should be avoided if unnecessary . Furthermore, patients may experience undue anxiety in the setting of a false-positive biopsy recommendation. Finally, the Z11 trial demonstrated that some patients with a low axillary burden (ie, no lymph node involvement or micrometastatic disease) do not benefit from axillary lymph node dissection when treated with whole-breast radiotherapy and systemic therapy . As a result, it is less important to biopsy cases with borderline abnormal lymph nodes, which at worst have micrometastatic disease. In current practice, radiologists will recommend biopsy of an axillary lymph node based on imaging features, including nodal size and cortical thickness.
Although lymph nodes may become completely replaced by cancer and grow very large, the first sign of malignant involvement is an increase in the cortical thickness . Several authors have proposed various cortical thickness thresholds to predict malignancy, aimed at maximizing sensitivity at the cost of specificity . These thresholds range from 2.3 mm to 3 mm, which typically achieve a sensitivity of greater than 90% . However, none of these published series included any information on the race and ethnicity of their study population. Imaging features of normal axillary lymph nodes, such as cortical thickness, may differ between women of different race and ethnicity, which could impact measurement thresholds used by radiologists to decide if biopsy should be recommended. Therefore, the purpose of this study was to determine if imaging features of normal axillary lymph nodes differ between black and white women.
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Schwab F.D., Burger H., Isenschmid M., et. al.: Suspicious axillary lymph nodes in patients with unremarkable imaging of the breast. Eur J Obstet Gynecol Reprod Biol 2010; 150: pp. 88-91.
2. Abe H., Schmidt R.A., Sennett C.A., et. al.: US-guided core needle biopsy of axillary lymph nodes in patients with breast cancer: why and how to do it. Radiographics 2007; 27: pp. S91-S99.
3. Vijayaraghavan G.R., Vedantham S., Kataoka M., et. al.: The relevance of ultrasound imaging of suspicious axillary lymph nodes and fine-needle aspiration biopsy in the post-ACOSOG Z11 era in early breast cancer. Acad Radiol 2017; 24: pp. 308-315.
4. Giuliano A.E., McCall L., Beitsch P., et. al.: Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial. Ann Surg 2010; 252: pp. 426-432. discussion 432-423
5. Bedi D.G., Krishnamurthy R., Krishnamurthy S., et. al.: Cortical morphologic features of axillary lymph nodes as a predictor of metastasis in breast cancer: in vitro sonographic study. AJR Am J Roentgenol 2008; 191: pp. 646-652.
6. Mainiero M.B.: Regional lymph node staging in breast cancer: the increasing role of imaging and ultrasound-guided axillary lymph node fine needle aspiration. Radiol Clin North Am 2010; 48: pp. 989-997.
7. Alvarez S., Anorbe E., Alcorta P., et. al.: Role of sonography in the diagnosis of axillary lymph node metastases in breast cancer: a systematic review. AJR Am J Roentgenol 2006; 186: pp. 1342-1348.
8. Net J.M., Mirpuri T.M., Plaza M.J., et. al.: Resident and fellow education feature: US evaluation of axillary lymph nodes. Radiographics 2014; 34: pp. 1817-1818.
9. Deurloo E.E., Tanis P.J., Gilhuijs K.G., et. al.: Reduction in the number of sentinel lymph node procedures by preoperative ultrasonography of the axilla in breast cancer. Eur J Cancer 2003; 39: pp. 1068-1073.
10. Cho N., Moon W.K., Han W., et. al.: Preoperative sonographic classification of axillary lymph nodes in patients with breast cancer: node-to-node correlation with surgical histology and sentinel node biopsy results. AJR Am J Roentgenol 2009; 193: pp. 1731-1737.
11. Mainiero M.B., Cinelli C.M., Koelliker S.L., et. al.: Axillary ultrasound and fine-needle aspiration in the preoperative evaluation of the breast cancer patient: an algorithm based on tumor size and lymph node appearance. AJR Am J Roentgenol 2010; 195: pp. 1261-1267.
12. Baltzer P.A., Dietzel M., Burmeister H.P., et. al.: Application of MR mammography beyond local staging: is there a potential to accurately assess axillary lymph nodes? Evaluation of an extended protocol in an initial prospective study. AJR Am J Roentgenol 2011; 196: pp. W641-W647.
13. Centers for Disease Control and Prevention. Breast Cancer Rates by Race and Ethnicity. Available at: https://www.cdc.gov/cancer/breast/statistics/race.htm . Accessed 7/31/17.
14. Guth A.A., Chun Kim J., Schwartz S., et. al.: The relationship of race, oncotype DX, and Ki67 in a population highly screened for breast cancer. Breast J 2017; 23: pp. 177-181.
15. Wieder R., Shafiq B., Adam N.: African American race is an independent risk factor in survival from initially diagnosed localized breast cancer. J Cancer 2016; 7: pp. 1587-1598.
16. Akinyemiju T.F., Vin-Raviv N., Chavez-Yenter D., et. al.: Race/ethnicity and socio-economic differences in breast cancer surgery outcomes. Cancer Epidemiol 2015; 39: pp. 745-751.
17. McCarthy A.M., Keller B.M., Pantalone L.M., et. al.: Racial differences in quantitative measures of area and volumetric breast density. J Natl Cancer Inst 2016; 108:
18. Nie K., Su M.Y., Chau M.K., et. al.: Age- and race-dependence of the fibroglandular breast density analyzed on 3D MRI. Med Phys 2010; 37: pp. 2770-2776.