
Rationale and Objectives
To document the frequency of normal and anomalous drainage patterns of the pulmonary veins, and to establish normal values for pulmonary vein ostial diameters, and distance to first bifurcation using multidetector computed tomography, as pertinent to ablation procedures for atrial fibrillation.
Materials and Methods
Two cardiothoracic radiologists retrospectively reviewed thin-section contrast material–enhanced multidetector computed tomography examinations of the thorax in 200 consecutive patients (38 females and 162 males), age 24–79 years (mean 52.8) referred for imaging before radiofrequency ablation therapy for atrial fibrillation. Pulmonary vein anatomy was based on both the number of venous ostia and the drainage patterns of pulmonary veins. Pulmonary vein ostial diameters and distance to first bifurcation of the four major pulmonary veins (right inferior and superior, left inferior and superior) and any additional pulmonary veins were measured at a workstation using both axial images and multiplanar reconstructions by two experienced cardiothoracic radiologists; the mean pulmonary vein diameter and the shortest distance to first bifurcation of the two measurements are reported.
Results
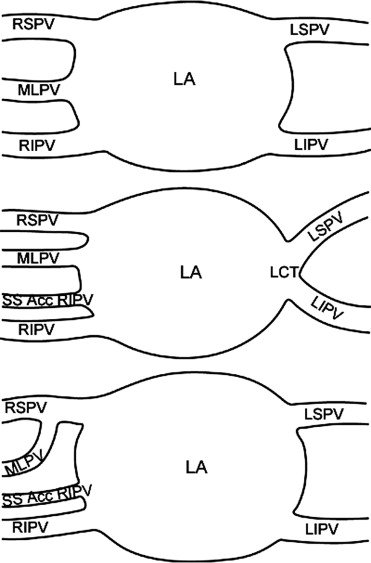
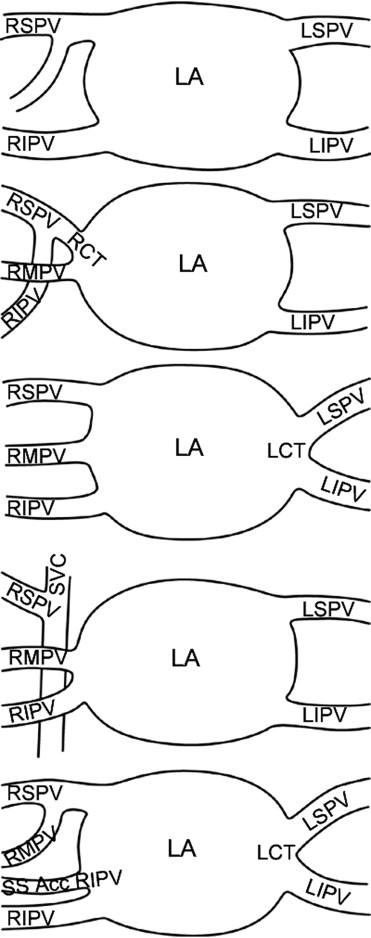
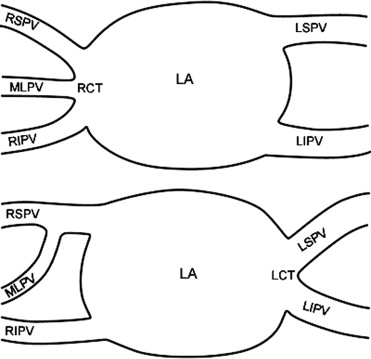
The majority of patients, 82% (164 patients) had four pulmonary veins, with a superior and inferior ostium on the right and a superior and inferior ostium on the left. Of the remainder, 9% (18 patients) had five veins, 4.5% (9 patients) had three veins, 3% (6 patients) had two anomalies each, and 0.5% (1 patient) had three anomalies. The middle lobe pulmonary vein drained into the right superior pulmonary vein in 83.5% of patients, directly into the left atrium in 11% of patients, and into the right inferior pulmonary vein in 5.5% of patients; 6.5% of patients had a single left pulmonary vein ostium. Mean pulmonary vein diameters with 95% confidence intervals at the ostia were as follows: right superior 17.6 (13.64–15.36) mm; left superior 16.6 (16.03–17.08) mm; right inferior 17.1 (16.58–17.55) mm; left inferior 14.8 (14.25–15.27) mm, and independent middle lobe 8.6 (8.27–8.86) mm. Mean distance to first bifurcation with 95% confidence intervals were: right superior 14.5 (17.02–18.23) mm; left superior 17.6 (16.63–18.53) mm; right inferior 7.0 (6.49–7.46) mm; left inferior 13.5 (12.83–14.16) mm, and independent middle lobe 8.4 (7.7–9.17) mm.
Conclusion
Thin-section thoracic computed tomography demonstrates a greater variability of pulmonary venous drainage than previously described. There is greater variability of the right lung venous drainage compared to the left lung. Eighty-two percent of people have four standard pulmonary veins. There is significant variability in pulmonary vein diameter and distance to first bifurcation.
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia, and is a major cause of stroke ( ). Treatment is directed at three major objectives: controlling the ventricular response, preventing thromboembolism, and maintaining normal sinus rhythm ( ). In the past few years, radiofrequency ablation of the pulmonary veins has been performed to disconnect the pulmonary veins electrically from the left atrium. Knowledge of ostial diameter facilitates catheter size selection during the ablation procedure. Furthermore, because pulmonary vein narrowing is critically dependent on catheter proximity to a bifurcation and not on duration of radiofrequency energy application, knowledge of the distance from each ostium to the first bifurcation of each pulmonary vein is important to prevent postablation pulmonary vein stenosis ( ). The purpose of our study was twofold: to establish the normative distribution of pulmonary venous drainage and categorize anatomic variations in venous drainage, and to establish normative values for pulmonary vein ostial diameters and distance to first pulmonary venous bifurcation.
Materials and methods
Subjects
Two hundred consecutive pulmonary vein mapping computed tomography (CT) examinations performed before radiofrequency ablation therapy for atrial fibrillation were retrospectively reviewed by two cardiothoracic radiologists. Of the 200 subjects (38 women and 162 men), women ranged in age from 24 to 73 years (mean age 56.8 years), and men ranged in age from 28 to 79 years (mean age 51.8 years). There was no statistically significant difference in ages between genders. This study was approved by our institutional review board.
Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Pulmonary Vein Anatomy
Get Radiology Tree app to read full this article<
Table 1a
Pulmonary Venous Drainage Patterns by Total Number of Pulmonary Veins
Number with 6 veins or more = 0 Number with 5 veins = 21 18 = Normal + MLPV 1 = MLPV + accessory RIPV + CLT 2 = Normal + accessory RIPV Number with 4 veins = 170 164 = Normal 1 = RCT + MLPV draining into LA 1 = LCT + MLPV draining into LA 1 = RSPV to SVC + MLPV draining into LA 3 = CLT + accessory RIPV Number with 3 veins = 9 1 = CRT 8 = CLT Number with 2 veins or less = 0
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1b
Pulmonary Venous Drainage Patterns by Number of Pulmonary Veins Separated by Side
Number of Right Veins Number of Left Veins Number with greater than 4 veins = 0 Number with greater than 4 veins = 0 Number with 4 veins = 1 Number with 4 veins = 0 1 = MLPV + accessory RIPV + CLT Number with 3 veins = 24 Number with 3 veins = 0
Number with 2 veins = 174 Number with 2 veins = 187
Number with 1 vein = 1 Number with 1 vein = 13 1 = CRT 8 = CLT 3 = CLT + accessory RIPV 1 = MLPV + accessory RIPV + CLT 1 = CLT + MLPV draining into LA
RSPV: right superior pulmonary vein; RIPV: right inferior pulmonary vein; LSPV: left superior pulmonary vein; LIPV: left inferior pulmonary vein; MLPV: middle lobe pulmonary vein; LA: left atrium; CRT: common right trunk; CLT: common left trunk; Acc RIPV: accessory right inferior pulmonary vein; SVC: superior vena cava.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Pulmonary Vein Ostial Diameter
Get Radiology Tree app to read full this article<
Table 2
Comparison of Pulmonary Vein Ostial Diameters by Gender
Mean Pulmonary Vein Diameter_P_ Value Men Women Right superior pulmonary vein 17.8 16.7 .13 Left superior pulmonary vein 16.7 15.9 .13 Middle lobe pulmonary vein 8.6 8.2 .14 Right inferior pulmonary vein 17.3 15.9 .04 Left inferior pulmonary vein 15.1 13.4 .007
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Mean Pulmonary Vein Ostial Diameters
Superior and Inferior Pulmonary Vein Ostial Diameters (mm) Minimum Mean Maximum SD 95% CI All SPV 6.00 17.00 30.00 4.12 16.70–17.50 RSPV 6.00 17.63 30.00 4.36 17.02–18.23 LSPV 9.00 16.56 26.70 3.80 16.03–17.08 All IPV 5.20 15.90 28.20 3.78 15.50–16.30 RIPV 8.50 17.06 28.20 3.50 16.58–17.55 LIPV 5.20 14.76 23.50 3.70 14.25–15.27
Middle Lobe Pulmonary Vein Ostial Diameter (mm) Minimum Mean Maximum SD 95% CI All MLPV 3.00 8.56 14.00 2.16 8.27–8.86 Drain to RSPV 3.00 8.50 14.00 2.10 8.27–8.82 Drain to RIPV 5.00 8.82 13.00 2.09 7.58–10.05 Drain to LA 4.00 8.60 14.00 2.67 7.50–9.73
Other Pulmonary Vein Ostial Diameters (mm) Minimum Mean Maximum SD 95% CI Common trunks 12.00 24.29 44.00 7.45 20.52–28.06 Accessory veins 6.00 7.70 9.70 1.44 6.60–8.91
SD: standard deviation; RSPV: right superior pulmonary vein; LSPV: left superior pulmonary vein; MLPV: middle lobe pulmonary vein; RIPV: right inferior pulmonary vein; LIPV: left inferior pulmonary vein.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Comparison of Pulmonary Vein Ostial Diameters
Pulmonary Vein Diameter Comparison Means (mm)P Value All SPV vs. All IPV
<.001 All SPV vs. ML PV
<.001 All IPV vs. ML PV
<.001 RSPV vs. RIPV
.15 RSPV vs. MLPV
<.001 RIPV vs. MLPV
<.001 LSPV vs. LIPV
<.001 RSPV vs. LSPV
.009 RIPV vs. LIPV
<.001 MLPV drains to RSPV vs. MLPV drains to RIPV
.68 MLPV drains to RSPV vs. MLPV drains to LA
.90 MLPV drains to RIPV vs. MLPV drains to LA
.81 Common trunk vs. all SPV
<.001 Common trunk vs. all IPV
<.001 Common trunk vs. RSPV
<.001 Common trunk vs. RIPV
<.001 Common trunk vs. LSPV
<.001 Common trunk vs. LIPV
<.001 Accessory PV vs. all SPV
<.001 Accessory PV vs. all IPV
<.001 Accessory PV vs. RSPV
<.001 Accessory PV vs. RIPV
<.001
All SPV: all superior pulmonary vein; all IPV: all inferior pulmonary vein; RSPV: right superior pulmonary vein; LSPV: left superior pulmonary vein; MLPV: middle lobe pulmonary vein; RIPV: right inferior pulmonary vein; LIPV: left inferior pulmonary vein.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Distance to First Bifurcation
Get Radiology Tree app to read full this article<
Table 5
Distance from Ostium to First Bifurcation of Pulmonary Veins
Superior and Inferior Pulmonary Vein Distance to First Bifurcation (mm) Minimum Mean Maximum SD 95% CI All SPV 1.00 16.00 43.00 6.70 15.30–16.70 RSPV 1.00 14.50 36.00 6.21 13.64–15.36 LSPV 1.60 17.58 43.00 6.48 16.63–18.53 All IPV 0.30 10.20 30.00 5.32 9.70–10.70 RIPV 0.30 6.97 21.00 3.51 6.49–7.46 LIPV 0.80 13.50 30.00 4.80 12.83–14.16 MLPV 1.00 8.43 29.00 5.31 7.70–9.17
Other Pulmonary Vein Distance to First Bifurcation (mm) Minimum Mean Maximum SD 95% CI Common trunks 1.00 9.76 26.00 7.10 6.16–13.35 Accessory veins 2.00 7.71 17.00 5.43 3.37–12.06
RSPV: right superior pulmonary vein; LSPV: left superior pulmonary vein; MLPV: middle lobe pulmonary vein; RIPV: right inferior pulmonary vein; LIPV: left inferior pulmonary vein.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 6
Comparison of Pulmonary Vein Distance To First Bifurcation
Distance to First Bifurcation Comparison Means (mm)P Value All SPV vs. All IPV
<.001 All SPV vs. ML PV
<.001 All IPV vs. ML PV
<.001 RSPV vs. RIPV
<.001 RSPV vs. MLPV
<.001 RIPV vs. MLPV
.001 LSPV vs. LIPV
<.001 RSPV vs. LSPV
<.001 RIPV vs. LIPV
<.001 Common trunk vs. All SPV
.008 Common trunk vs. All IPV
.96 Common trunk vs. RSPV
.043 Common trunk vs. RIPV
.089 Common trunk vs. LSPV
.002 Common trunk vs. LIPV
.11 Accessory PV vs. all SPV
.02 Accessory PV vs. all IPV
.51 Accessory PV vs. RSPV
.046 Accessory PV vs. RIPV
.48
All SPV: all superior pulmonary vein; all IPV: all inferior pulmonary vein; RSPV: right superior pulmonary vein; LSPV: left superior pulmonary vein; MLPV: middle lobe pulmonary vein; RIPV: right inferior pulmonary vein; LIPV: left inferior pulmonary vein.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Haissaguerre M., Jais P., Shah D.C., et. al.: Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998; 339: pp. 659-666.
2. Pelosi F., Morady F.: Evaluation and management of atrial fibrillation. Med Clin North Am 2001; 85: pp. 225-244.
3. Scharf C., Sneider M., Case I., et. al.: Anatomy of the pulmonary veins in patients with atrial fibrillation and effects of segmental ostial ablation analyzed by computed tomography. J Cardiovasc Electrophysiol 2003; 14: pp. 150-155.
4. Cronin P., Sneider M.B., Kazerooni E.A., et. al.: Multislice CT imaging of the left atrium and pulmonary veins in planning radiofrequency ablation for atrial fibrillation: a how to guide. AJR Am J Roentgenol 2004; 183: pp. 767-778.
5. Shah D.C., Haissaguerre M., Jais P., et. al.: Electrophysiologically guided ablation of the pulmonary veins for the curative treatment of atrial fibrillation. Ann Med 2000; 32: pp. 408-416.
6. Ho S.Y., Sanchez-Quintana D., Cabrera J.A., et. al.: Anatomy of the left atrium: implications for radiofrequency ablation of atrial fibrillation. J Cardiovasc Electrophysiol 1999; 10: pp. 1525-1533.
7. Ho S.Y., Cabrera J.A., Tran V.H., et. al.: Architecture of the pulmonary veins: relevance to radiofrequency ablation. Heart 2001; 86: pp. 265-270.
8. Alfke H., Wagner H.J., Klose K.J.: A case of an anomalous pulmonary vein of the right middle lobe. Cardiovasc Intervent Radiol 1995; 18: pp. 406-409.
9. Collins D.R., Shea P.M., Vieweg W.V.: Idiopathic prominence of pulmonary veins on chest Xray. Angiology 1982; 33: pp. 613-616.
10. Benfield J.R., Gots R.E., Mills D.: Anomalous single left pulmonary vein mimicking a parenchymal nodule. Chest 1971; 59: pp. 101-103.
11. Hasuo K., Numaguchi Y., Kishikawa T., et. al.: Anomalous unilateral single pulmonary vein mimicking pulmonary varices. Chest 1981; 79: pp. 602-604.
12. Tretheway D.G., Francis G.S., MacNeil D.J., et. al.: Single left pulmonary vein with normal pulmonary venous drainage: a roentgenographic curiosity. Am J Cardiol 1974; 34: pp. 237-239.
13. Rey C., Vaksmann G., Francart C.: Anomalous unilateral single pulmonary vein mimicking partial anomalous pulmonary venous return. Cathet Cardiovasc Diagn 1986; 12: pp. 330-333.
14. Mangrum J.M., Mounsey J.P., Kok L.C., et. al.: Intracardiac echocardiography-guided, anatomically based radiofrequency ablation of focal atrial fibrillation originating from pulmonary veins. J Am Coll Cardiol 2002; 39: pp. 1964-1972.
15. Marom E.M., Herndon J.E., Kim Y.H., et. al.: Variations in pulmonary venous drainage to the left atrium: implications for radiofrequency ablation. Radiology 2004; 230: pp. 824-829.
16. Mansour M., Holmvang G., Sosnovik D., et. al.: Assessment of pulmonary vein anatomic variability by magnetic resonance imaging: implications for catheter ablation techniques for atrial fibrillation. J Cardiovasc Electrophysiol 2004; 15: pp. 387-393.
17. Ghaye B., Szapiro D., Dacher J.N., et. al.: Percutaneous ablation for atrial fibrillation: the role of cross-sectional imaging. Radiographics 2003; 23: pp. S19-S33.
18. Kato R., Lickfett L., Meininger G., et. al.: Pulmonary vein anatomy in patients undergoing catheter ablation of atrial fibrillation: lessons learned by use of magnetic resonance imaging. Circulation 2003; 107: pp. 2004-2010.
19. Yuan X.P., Bach D., Skanes A., et. al.: Assessment of intra- and interobserver variability of pulmonary vein measurements from CT angiography. Acad Radiol 2004; 11: pp. 1211-1218.
20. Schwartzman D., Lacomis J., Wigginton W.G.: Characterization of left atrium and distal pulmonary vein morphology using multidimensional computed tomography. J Am Coll Cardiol 2003; 41: pp. 1349-1357.
21. Kim Y.H., Marom E.M., Herndon J.E., et. al.: Pulmonary vein diameter, cross-sectional area, and shape: CT analysis. Radiology 2005; 235: pp. 43-49.
22. Tsao H.M., Wu M.H., Yu W.C., et. al.: Role of right middle pulmonary vein in patients with paroxysmal atrial fibrillation. J Cardiovasc Electrophysiol 2001; 12: pp. 1353-1357.
23. Lin W.S., Prakash V.S., Tai C.T., et. al.: Pulmonary vein morphology in patients with paroxysmal atrial fibrillation initiated by ectopic beats originating from the pulmonary veins: implications for catheter ablation. Circulation 2000; 101: pp. 1274-1281.