
Rationale and Objectives
To assess patient radiation dose reduction and the image quality of a new X-ray imaging technology during repetitive transarterial chemoembolization (TACE) for hepatocellular carcinoma (HCC).
Methods
Fifty HCC patients (36 men; 57 ± 11 years) undergoing repetitive TACE were first randomly assigned to receive a TACE treatment on a reference X-ray system or a low-dose system with advanced real-time image processing. The alternate system was used for a repeated TACE (treatment interval, 0.5–6 months). Fluoroscopy time, number of digital subtraction angiography (DSA), air kerma (AK), and dose area product (DAP) were compared between the two systems and between the two repetitive TACE. Three interventional radiologists independently rated the image quality in blinded offline readings.
Results
Fluoroscopy time (8.7 ± 5.9 minutes vs. 8.7 ± 7.9 minutes, P = .981), numbers of DSA runs (6 ± 4 vs. 6 ± 4, P = .735), and exposure images (173 ± 86 vs. 168 ± 91, P = .916) were equivalent between the two systems. No statistical difference in X-ray usage was found between repeated treatments. Compared to the reference system, the technology significantly reduced AK and DAP by 48.6% (0.17 ± 0.13 Gy vs. 0.41 ± 0.36 Gy, P < .0001) and 50.3% (77.3 ± 55.2 Gy cm 2 vs. 195.0 ± 155.5 Gy cm 2 , P < .0001), respectively. Image quality was rated comparable between the new system and the reference, with average scores of 3.9 ± 0.3 versus 4.4 ± 0.3 in fluoroscopy and 4.5 ± 0.2 versus 4.3 ± 0.3 in DSA.
Conclusions
Patient radiation exposure can be substantially reduced by a factor of approximately two with the novel X-ray imaging technology while maintaining image quality.
Introduction
Patients with unresectable hepatocellular carcinoma (HCC) can receive transarterial chemoembolization (TACE) as a palliative treatment . However, guided by fluoroscopy and digital subtraction angiography (DSA), the interventional radiologic procedure could result in a considerable amount of radiation which may put the patient at risk to radiation-induced skin injuries. Furthermore, because of tumor recurrence, repetitive embolization is often required , increasing the burden of cumulative radiation exposure to the patient and the clinical stuff.
In accordance with the “as low as reasonably achievable” (ALARA) principle, radiation dose should be kept at the lowest possible level when conducting radiologic procedures. However, during TACE therapies, clinically sufficient image quality might be obtained at the expense of radiation dose due to the X-ray attenuation while penetrating the abdomen during image acquisitions. Furthermore, noise and artifacts in the images, caused by breathing for instance, may necessitate additional image acquisition and increase patient irradiation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Table 1
Patient Baseline Characteristics
Age, y ∗ 57 ± 11 Sex Male 36 Female 14 Body mass index (kg/m 2 ) ∗ 23.0 ± 3.2 Repetitive TACE indication Local lipiodol loss 45 Local lesion recurrence 6 New lesion appearance 3 Treatment interval (d) † 50 (11–224)
Assessment 1 (n = 50) Assessment 2 (n = 50) Child–Pugh Score A 34 31 B 16 19 C 0 0 Barcelona clinical liver cancer staging 0 5 5 A 12 12 B 25 25 C 8 8 D 0 0
TACE, transarterial chemoembolization.
Except where indicated, data represent numbers of patients.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Technology
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Quality Assessment
Get Radiology Tree app to read full this article<
Table 2
Image Quality Scoring Scale Used to Assess Fluoroscopy
Score Hepatic Artery Visibility to Sub-subsegmental Level Branches Intravascular Lipiodol Flow Direction and Speed Visibility Tumor Lipiodol Deposition Visibility 5 Clear Clear Clear 4 Clear Clear Fair 3 Clear Fair Fair 2 Subsegmental level, fair; sub-subsegmental level, poor Poor Poor 1 Subsegmental level, poor; sub-subsegmental level, not visible Poor Not visible 0 Not visible Not visible Not visible
Table 3
Image Quality Scoring Scale Used to Assess Digital Subtraction Angiography
Score Hepatic Artery Visibility to Sub-subsegmental Level Branches Tumor (Size, Border) and Feeding Vessel Visibility Portal Vein Visibility 5 Clear Clear Clear 4 Clear Tumor, clear; feeding vessel, fair Clear 3 Clear Fair Fair 2 Subsegmental level, clear; sub-subsegmental level, fair Poor Fair 1 Subsegmental level, clear; sub-subsegmental level, poor Tumor, poor; feeding vessel, not visible Not visible 0 Not visible Not visible Not visible
Get Radiology Tree app to read full this article<
Data Collection and Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
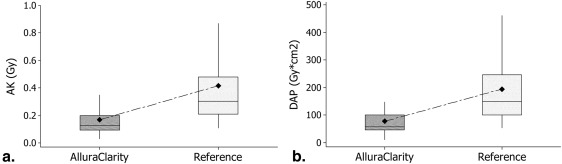
Table 4
Procedural X-Ray Usage and Patient Radiation Dose
AlluraClarity (n = 50) Reference (n = 50) Average Reduction (%)P Value Fluoroscopy time (min) 8.7 ± 5.9 8.7 ± 7.9 NS DSA runs 6 ± 4 6 ± 4 NS Exposure images 173 ± 86 168 ± 91 NS Total AK (Gy) 48.6 <.0001 Mean ± SD 0.17 ± 0.13 0.41 ± 0.36 Median (Q1–Q3) 0.13 (0.09–0.20) 0.30 (0.21–0.48) AK–fluoroscopy (Gy) <.0001 Mean ± SD 0.05 ± 0.04 0.12 ± 0.10 Median (Q1–Q3) 0.03 (0.02–0.06) 0.08 (0.07–0.14) AK–DSA (Gy) <.0001 Mean ± SD 0.12 ± 0.09 0.30 ± 0.29 Median (Q1–Q3) 0.09 (0.06–0.15) 0.22 (0.15–0.31) Total DAP (Gy∙cm 2 ) 50.3 <.0001 Mean ± SD 77.3 ± 55.2 195.0 ± 155.5 Median (Q1–Q3) 57.4 (45.5–101.0) 149.5 (100.6–245.8) DAP–fluoroscopy (Gy∙cm 2 ) <.0001 Mean ± SD 21.8 ± 17.7 53.4 ± 43.8 Median (Q1–Q3) 15.7 (11.3–27.2) 38.1 (25.7–58.9) DAP–DSA (Gy∙cm 2 ) <.0001 Mean ± SD 55.5 ± 40.4 141.5 ± 127.2 Median (Q1–Q3) 43.3 (29.3–72.4) 114.1 (72.8–155.7)
AK, air kerma; DAP, dose area product; DSA, digital subtraction angiography; NS, not significant; Q1–Q3, first to third quartile range; SD, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Arii S., Yamaoka Y., Futagawa S., et. al.: Results of surgical and nonsurgical treatment for small-sized hepatocellular carcinomas: a retrospective and nationwide survey in Japan. The Liver Cancer Study Group of Japan. Hepatology 2000; 32: pp. 1224-1229.
2. Takayasu K., Arii S., Ikai I., et. al., Liver Cancer Study Group of Japan: Prospective cohort study of transarterial chemoembolization for unresectable hepatocellular carcinoma in 8510 patients. Gastroenterology 2006; 131: pp. 461-469.
3. Llovet J.M., Bruix J.: Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology 2003; 37: pp. 429-442.
4. Bruix J., Sherman M.: Management of hepatocellular carcinoma: an update. Hepatology 2011; 53: pp. 1020-1022.
5. European Association for the Study of the Liver, European Organisation for Research and Treatment of Cancer: EASL–EORTC clinical practice guidelines: management of hepatocellular carcinoma. Journal of Hepatology 2012; 56: pp. 908-943.
6. Miller D.L., Balter S., Cole P.E., et. al.: Radiation doses in interventional radiology procedures: the RAD-IR study, Part I: overall measures of dose. J Vasc Interv Radiol 2003; 14: pp. 711-727.
7. Miller D., Kwon D., Bonavia G.H.: Reference levels for patient radiation doses in interventional radiology: proposed initial values for U.S. practice. Radiology 2009; 253: pp. 753-764.
8. Hidajat N., Wust P., Felix R., et. al.: Radiation exposure to patient and staff in hepatic chemoembolization: risk estimation of cancer and deterministic effects. Cardiovasc Intervent Radiol 2006; 29: pp. 791-796.
9. Livingstone R.S., Mammen T., GOPI : Evaluation of radiation dose to patients during abdominal embolizations. Indian J Med Sci 2005; 59: pp. 527-533.
10. Vogl T.J., Naguib N.N., Nour-Eldin N.E., et. al.: Retrospective study on the use of different protocols for repeated transarterial chemoembolization in the treatment of patients with hepatocellular carcinoma. Acad Radiol 2012 Apr; 19: pp. 434-439.
11. Vogl T.J., Gruber-Rouh T., Eichler K., et. al.: Repetitive transarterial chemoembolization (TACE) of liver metastases from gastric cancer: local control and survival results. Eur J Radiol 2013; 82: pp. 258-263.
12. Azizi A., Naguib N.N., Mbalisike E., et. al.: Liver metastases of pancreatic cancer: role of repetitive transarterial chemoembolization (TACE) on tumor response and survival. Pancreas 2011; 40: pp. 1271-1275.
13. Dekker L.R., van der Voort P.H., Simmers T.A., et. al.: New image processing and noise reduction technology allows reduction of radiation exposure in complex electrophysiologic interventions while maintaining optimal image quality: a randomized clinical trial. Heart Rhythm 2013; 10: pp. 1678-1682.
14. Söderman M., Holmin S., Andersson T., et. al.: Image noise reduction algorithm for digital subtraction angiography: clinical results. Radiology 2013; 269: pp. 553-560.
15. Racadio J., Strauss K., Abruzzo T., et. al.: Significant dose reduction for pediatric digital subtraction angiography without impairing image quality: preclinical study in a piglet model. AJR 2014; 203: pp. 904-908.
16. Van Strijen M.J., Grünhagen T., Mauti M., et. al.: Evaluation of a noise reduction imaging technology in iliac digital subtraction angiography: noninferior clinical image quality with lower patient and scatter dose. J Vasc Interv Radiol 2015 Mar;
17. Söderman M., Mauti M., Boon S., et. al.: Radiation dose in neuroangiography using image noise reduction technology: a population study based on 614 patients. Neuroradiology 2013; 55: pp. 1365-1372.
18. Nakamura S., Kobayashi T., Funatsu A., et. al.: Patient radiation dose reduction using an X- ray imaging noise reduction technology for cardiac angiography and intervention. Heart Vessels 2015 Apr 4;
19. Jago J., Collet-Billon A., Chenal C., et. al.: XRES®: adaptive enhancement of ultrasound images. Medicamundi 2002; 46: pp. 36-41.
20. Meuwly JY,Thiran JP,Gudinchet F. Application of adaptive image processing technique to real-time spatial compound ultrasound