
Rationale and Objectives
In patients with severe emphysema and poor quality of life, bronchoscopic lung volume reduction (BLVR) may be considered and guided based on lobar emphysema severity. In particular, x-ray computed tomography (CT) emphysema measurements are used to identify the most diseased and the second–most diseased lobes as BLVR targets. Inhaled gas magnetic resonance imaging (MRI) also provides chronic obstructive pulmonary disease (COPD) biomarkers of lobar emphysema and ventilation abnormalities. Our objective was to retrospectively evaluate CT and MRI biomarkers of lobar emphysema and ventilation in patients with COPD eligible for BLVR. We hypothesized that MRI would provide complementary biomarkers of emphysema and ventilation that help determine the most appropriate lung lobar targets for BLVR in patients with COPD.
Materials and Methods
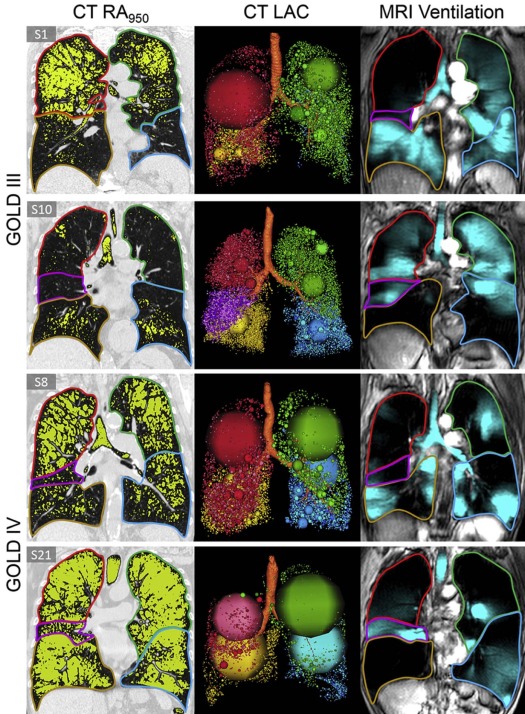
We retrospectively evaluated 22 BLVR-eligible patients from the Thoracic Imaging Network of Canada cohort (diffusing capacity of the lung for carbon monoxide = 37 ± 12% predicted , forced expiratory volume in 1 second = 34 ± 7% predicted , total lung capacity = 131 ± 17% predicted , and residual volume = 216 ± 36% predicted ). Lobar CT emphysema, measured using a relative area of <−950 Hounsfield units (RA 950 ) and MRI ventilation defect percent, was independently used to rank lung lobe disease severity.
Results
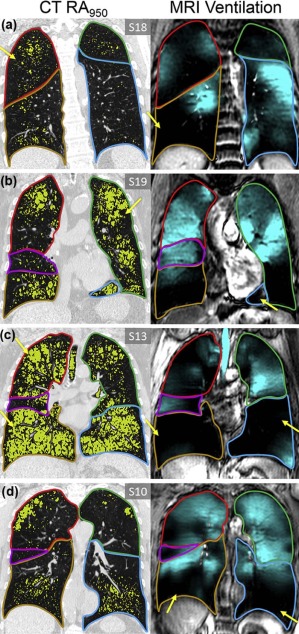
In 7 of 22 patients, there were different CT and MRI predictions of the most diseased lobe. In some patients, there were large ventilation defects in lobes not targeted by CT, indicative of a poorly ventilated lung. CT and MRI classification of the most diseased and the second–most diseased lobes showed a fair-to-moderate intermethod reliability (Cohen κ = 0.40–0.59).
Conclusions
In this proof-of-concept retrospective analysis, quantitative MRI ventilation and CT emphysema measurements provided different BLVR targets in over 30% of the patients. The presence of large MRI ventilation defects in lobes next to CT-targeted lobes might also change the decision to proceed or to guide BLVR to a different lobar target.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by a chronic airflow limitation associated with airway inflammation due to long-term exposure to inhaled toxins and particles . In patients with COPD, emphysematous tissue destruction and narrowing of the small airways contribute to airflow limitation , lung hyperinflation, dyspnea, and worsening quality of life . Emphysema is inexorably progressive and irreversible, whereas lung hyperinflation also worsens over time and leads to worsening lung compliance, loss of exercise capacity, increased frequency of exacerbations, and a significant decline in quality of life . To improve symptoms and quality of life in patients with very severe COPD and extensive emphysema, lung volume reduction techniques were developed to selectively reduce or remove emphysematous tissue .
The overarching goal of lung volume reduction methods is to improve lung function and to decrease hyperinflation, which together result in improved patient quality of life and functional status . Such surgical approaches, however, are associated with significant morbidity and mortality . However, in a specific subgroup of patients with heterogeneous upper lobe predominant emphysema and poor functional status, there were significant benefits , including modest improvements in quality of life . Since then, a number of minimally invasive bronchoscopic lung volume reduction (BLVR) approaches have been developed with the goal of improving outcomes and diminished morbidity and mortality associated with the procedure. Several methods have been pioneered, including coils to collapse large airways , one-way endobronchial valves to promote passive collapse and deflation over time , and thermal vapor ablation to create an inflammatory response with subsequent scarring and loss of volume . Collateral ventilation is an important determinant of optimal BLVR outcomes , although recent studies showed that BLVR using vapor ablation may be successful regardless of interlobar or intralobar collateral ventilation . For all of these approaches, typically one or two severely diseased lobes are targeted with the aim of diverting blood flow and ventilation to remaining areas of healthier lung parenchymas .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Study Subjects
Get Radiology Tree app to read full this article<
Pulmonary Function Tests
Get Radiology Tree app to read full this article<
Image Acquisition
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
DSC=2|VDP∩RA950||VDP|+|RA950| D
S
C
=
2
|
V
D
P
∩
R
A
950
|
|
V
D
P
|
+
|
R
A
950
|
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistics
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Subject Demographic and Pulmonary Function Measurements
Mean (±SD) All ( n = 22) Age (y) 69 (9) Male, n 14 BMI (kg/m 2 ) 25 (4) Pack-year history (y) 60 (35) FEV 1 , % pred 34 (7) FVC, % pred 74 (17) FEV 1 /FVC (%) 46 (9) TLC, % pred 131 (17) RV, % pred 216 (36) RV/TLC (%) 164 (18) R AW , % pred 304 (126) DL CO , % pred 37 (12) 6MWD (min) 325 (73) RA 950 (%) 20 (10) VDP (%) 33 (9) DSC (%) 29 (12) SOC RA950 (%) 40 (14)
% pred , percent of predicted value; 6MWD, 6-minute walk test distance; BMI, body mass index; DL CO , diffusing capacity for carbon monoxide; DSC, dice similarity coefficient; FEV 1 , forced expiratory volume in 1 second; FVC, forced vital capacity; RA 950 , relative area of computed tomography density histogram with attenuation values of <−950 HU; R AW , airways resistance; RV, residual volume; SD, standard deviation; SOC, spatial overlap coefficient normalized by RA 950 ; TLC, total lung capacity; VDP, ventilation defect percent.
Table 2
Participant Listing of Demographic and Other Measurements
Subject Age (y) FEV 1 , % pred TLC, % pred RV, % pred RV/TLC (%) DL CO , % pred RA 950 (%) VDP (%) DSC (%) SOC RA950 (%) 1 71 45 127 186 63 31 21 31 38 47 2 48 43 148 189 36 41 20 22 21 23 3 78 38 123 186 58 29 23 32 29 35 4 72 40 135 210 67 54 7 21 14 28 5 51 40 114 208 54 46 12 42 28 64 6 74 30 135 236 66 39 22 37 38 52 7 60 21 102 205 65 45 9 30 16 34 8 68 23 124 214 76 — 27 29 31 33 9 76 32 125 220 64 40 16 36 27 45 10 65 39 120 156 54 63 8 26 18 36 11 78 42 161 221 67 27 19 32 28 37 12 73 34 165 289 64 37 17 40 32 53 13 75 28 141 267 71 17 29 33 38 40 14 67 37 154 265 72 21 32 41 46 53 15 61 30 128 222 71 30 24 42 40 54 16 74 34 141 225 59 24 33 57 51 69 17 63 22 116 180 64 41 23 32 29 34 18 63 38 111 183 55 40 8 26 15 31 19 85 38 124 194 63 36 18 30 24 32 20 73 32 133 230 65 35 15 14 15 14 21 72 26 155 291 68 21 52 44 55 51 22 73 41 107 172 58 54 8 23 13 24 Mean (±SD) 69 (9) 34 (7) 131 (17) 216 (36) 63 (8) 37 (12) 20 (10) 33 (9) 29 (12) 40 (14)
% pred , percent of predicted value; DL CO , diffusing capacity for carbon monoxide; DSC, dice similarity coefficient; FEV 1 , forced expiratory volume in 1 second; RA 950 , relative area of computed tomography density histogram with attenuation values of <−950 HU; RV, residual volume; SD, standard deviation; SOC, spatial overlap coefficient normalized by RA 950 ; TLC, total lung capacity; VDP, ventilation defect percent.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
VDP and RA 950 Classification of Most Diseased Lobes by Participant
 Open full size image
Open full size image
LLL, left lower lobe; LUL, left upper lobe; MDL, most diseased lung lobe; RA 950 , relative area of computed tomography density histogram with attenuation values of <−950 HU; RLL, right lower lobe; RML, right middle lobe; RUL, right upper lobe; VDP, ventilation defect percent.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
VDP and RA 950 Agreement for Identifying and Ranking the Most Diseased Lobes
Most Diseased Lung Lobe VDP-RA 950 Agreement, N = 22 Cohen’s κ (Confidence Interval)P Value 1 15 (68%) 0.59 (0.35–0.83) <0.001 1 + 2 14 (64%) 0.55 (0.32–0.78) <0.001 2 12 (55%) 0.41 (0.14–0.68) <0.001 3 10 (46%) 0.30 (0.04–0.55) 0.007 4 11 (50%) 0.36 (0.23–0.48) 0.001 5 12 (55%) 0.38 (0.25–0.51) 0.001
RA 950 , relative area of computed tomography density histogram with attenuation values of <−950 HU; VDP, ventilation defect percent.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Supplementary Data
Get Radiology Tree app to read full this article<
Video S1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Hogg J.C., Chu F., Utokaparch S., et. al.: The nature of small-airway obstruction in chronic obstructive pulmonary disease. NEJM 2004; 350: pp. 2645-2653.
2. Pauwels R.A., Buist A.S., Calverley P.M., et. al.: Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2001; 163: pp. 1256-1276.
3. Hurst J.R., Vestbo J., Anzueto A., et. al.: Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med 2010; 363: pp. 1128-1138.
4. Thomas M., Decramer M., O’Donnell D.E.: No room to breathe: the importance of lung hyperinflation in COPD. Prim Care Respir J 2013; 22: pp. 101-111.
5. Herth F.J., Gompelmann D., Ernst A., et. al.: Endoscopic lung volume reduction. Respiration 2009; 79: pp. 5-13.
6. Deslee G., Klooster K., Hetzel M., et. al.: Lung volume reduction coil treatment for patients with severe emphysema: a European multicentre trial. Thorax 2014; 69: pp. 980-986.
7. Herth F.J., Valipour A., Shah P.L., et. al.: Segmental volume reduction using thermal vapour ablation in patients with severe emphysema: 6-month results of the multicentre, parallel-group, open-label, randomised controlled STEP-UP trial. Lancet Respir Med 2016; 4: pp. 185-193.
8. Brenner M., Yusen R., McKenna R., et. al.: Lung volume reduction surgery for emphysema. Chest 1996; 110: pp. 205-218.
9. Cooper J.D., Patterson G.A., Sundaresan R.S., et. al.: Results of 150 consecutive bilateral lung volume reduction procedures in patients with severe emphysema. J Thorac Cardiovasc Surg 1996; 112: pp. 1319-1329. discussion 29–30
10. Group NETTR.: Patients at high risk of death after lung-volume–reduction surgery. N Engl J Med 2001; 2001: pp. 1075-1083.
11. Koegelenberg C.F.N., Theron J., Bruwer J., et. al.: Endoscopic lung volume reduction in severe emphysema. S Afr Med J 2015; 105: pp. 721-723.
12. Naunheim K.S., Wood D.E., Mohsenifar Z., et. al.: Long-term follow-up of patients receiving lung-volume-reduction surgery versus medical therapy for severe emphysema by the National Emphysema Treatment Trial Research Group. Ann Thorac Surg 2006; 82: pp. 431-443.
13. Criner G.J., Cordova F., Sternberg A.L., et. al.: The National Emphysema Treatment Trial (NETT) part II: lessons learned about lung volume reduction surgery. Am J Respir Crit Care Med 2011; 184: pp. 881-893.
14. Davey C., Zoumot Z., Jordan S., et. al.: Bronchoscopic lung volume reduction with endobronchial valves for patients with heterogeneous emphysema and intact interlobar fissures (the BeLieVeR-HIFi study): a randomised controlled trial. Lancet 2015; 386: pp. 1066-1073.
15. Snell G., Herth F.J., Hopkins P., et. al.: Bronchoscopic thermal vapour ablation therapy in the management of heterogeneous emphysema. Eur Respir J 2012; 39: pp. 1326-1333.
16. Shah P.L., Zoumot Z., Singh S., et. al.: Endobronchial coils for the treatment of severe emphysema with hyperinflation (RESET): a randomised controlled trial. Lancet Respir Med 2013; 1: pp. 233-240.
17. Klooster K., ten Hacken N.H., Hartman J.E., et. al.: Endobronchial valves for emphysema without interlobar collateral ventilation. N Engl J Med 2015; 373: pp. 2325-2335.
18. Deslee G., Mal H., Dutau H., et. al.: Lung volume reduction coil treatment vs usual care in patients with severe emphysema: the REVOLENS Randomized Clinical Trial. JAMA 2016; 315: pp. 175-184.
19. Sciurba F.C., Ernst A., Herth F.J., et. al.: A randomized study of endobronchial valves for advanced emphysema. N Engl J Med 2010; 363: pp. 1233-1244.
20. Fishman A., Martinez F., Naunheim K., et. al.: A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med 2003; 348: pp. 2059-2073.
21. Gompelmann D., Eberhardt R., Ernst A., et. al.: The localized inflammatory response to bronchoscopic thermal vapor ablation. Respiration 2013; 86: pp. 324-331.
22. Herth F.J., Ernst A., Baker K.M., et. al.: Characterization of outcomes 1 year after endoscopic thermal vapor ablation for patients with heterogeneous emphysema. Int J Chron Obstruct Pulmon Dis 2012; 7: pp. 397-405.
23. Salerno M., de Lange E.E., Altes T.A., et. al.: Emphysema: hyperpolarized helium 3 diffusion MR imaging of the lungs compared with spirometric indexes—initial experience. Radiology 2002; 222: pp. 252-260.
24. de Lange E.E., Mugler J.P., Brookeman J.R., et. al.: Lung air spaces: MR imaging evaluation with hyperpolarized 3He gas. Radiology 1999; 210: pp. 851-857.
25. Mathew L., Kirby M., Etemad-Rezai R., et. al.: Hyperpolarized 3 He magnetic resonance imaging: preliminary evaluation of phenotyping potential in chronic obstructive pulmonary disease. Eur J Radiol 2011; 79: pp. 140-146.
26. Kirby M., Pike D., Coxson H.O., et. al.: Hyperpolarized (3)He ventilation defects used to predict pulmonary exacerbations in mild to moderate chronic obstructive pulmonary disease. Radiology 2014; 273: pp. 887-896.
27. Kirby M., Mathew L., Wheatley A., et. al.: Chronic obstructive pulmonary disease: longitudinal hyperpolarized 3He MR imaging 1. Radiology 2010; 256: pp. 280-289.
28. Parraga G., Ouriadov A., Evans A., et. al.: Hyperpolarized 3He ventilation defects and apparent diffusion coefficients in chronic obstructive pulmonary disease: preliminary results at 3.0 Tesla. Invest Radiol 2007; 42: pp. 384-391.
29. Kauczor H.-U., Hofmann D., Kreitner K.-F., et. al.: Normal and abnormal pulmonary ventilation: visualization at hyperpolarized He-3 MR imaging. Radiology 1996; 201: pp. 564-568.
30. Capaldi D.P.I., Zha N.X., Guo F.M., et. al.: Pulmonary imaging biomarkers of gas trapping and emphysema in COPD: He-3 MR imaging and CT parametric response maps. Radiology 2016; 279: pp. 597-608.
31. Kirby M., Svenningsen S., Owrangi A., et. al.: Hyperpolarized 3He and 129Xe MR imaging in healthy volunteers and patients with chronic obstructive pulmonary disease. Radiology 2012; 265: pp. 600-610.
32. Kirby M., Pike D., McCormack D.G., et. al.: Longitudinal computed tomography and magnetic resonance imaging of COPD: Thoracic Imaging Network of Canada (TINCan) study objectives. Chronic Obstr Pulm Dis 2014; 1: pp. 200-211.
33. Vestbo J., Hurd S.S., Agustí A.G., et. al.: Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med 2013; 187: pp. 347-365.
34. Schroeder J.D., McKenzie A.S., Zach J.A., et. al.: Relationships between airflow obstruction and quantitative CT measurements of emphysema, air trapping, and airways in subjects with and without chronic obstructive pulmonary disease. AJR Am J Roentgenol 2013; 201: pp. W460-W470.
35. Miller M.R., Hankinson J., Brusasco V., et. al.: Standardisation of spirometry. Eur Respir J 2005; 26: pp. 319-338.
36. Wanger J., Clausen J.L., Coates A., et. al.: Standardisation of the measurement of lung volumes. Eur Respir J 2005; 26: pp. 511-522.
37. Jones P.W., Quirk F.H., Baveystock C.M.: The St George’s Respiratory Questionnaire. Respir Med 1991; 85: pp. 25-31. discussion 3–7
38. Holland A.E., Spruit M.A., Troosters T., et. al.: An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. Eur Respir J 2014; 44: pp. 1428-1446.
39. Kirby M., Heydarian M., Svenningsen S., et. al.: Hyperpolarized 3 He magnetic resonance functional imaging semiautomated segmentation. Acad Radiol 2012; 19: pp. 141-152.
40. Sheikh K., Capaldi D.P., Hoover D.A., et. al.: Magnetic resonance imaging biomarkers of chronic obstructive pulmonary disease prior to radiation therapy for non-small cell lung cancer. Eur J Radiol Open 2015; 2: pp. 81-89.
41. Heinrich M.P., Jenkinson M., Bhushan M., et. al.: MIND: Modality Independent Neighbourhood Descriptor for multi-modal deformable registration. Med Image Anal 2012; 16: pp. 1423-1435.
42. Dice L.R.: Measures of the amount of ecologic association between species. Ecology 1945; 26: pp. 297-302.
43. Gietema H.A., Schilham A.M., van Ginneken B., et. al.: Monitoring of smoking-induced emphysema with CT in a lung cancer screening setting: detection of real increase in extent of emphysema. Radiology 2007; 244: pp. 890-897.
44. McHugh M.L.: Interrater reliability: the Kappa statistic. Biochem Med (Zagreb) 2012; 22: pp. 276-282.
45. Shah P.L., Herth F.J.: Current status of bronchoscopic lung volume reduction with endobronchial valves. Thorax 2014; 69: pp. 280-286.
46. Agusti A., Calverley P.M., Celli B., et. al.: Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res 2010; 11: pp. 122.
47. Martinez C.H., Chen Y.H., Westgate P.M., et. al.: Relationship between quantitative CT metrics and health status and BODE in chronic obstructive pulmonary disease. Thorax 2012; 67: pp. 399-406.
48. Gietema H.A., Edwards L.D., Coxson H.O., et. al.: Impact of emphysema and airway wall thickness on quality of life in smoking-related COPD. Respir Med 2013; 107: pp. 1201-1209.
49. Iwasaki A., Shirakusa T., Enatsu S., et. al.: Surgical treatment for lung cancer with COPD based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD). Thorac Cardiov Surg 2005; 53: pp. 162-167.
50. Palma D., Lagerwaard F., Rodrigues G., et. al.: Curative treatment of stage I non-small-cell lung cancer in patients with severe COPD: stereotactic radiotherapy outcomes and systematic review. Int J Radiat Oncol Biol Phys 2012; 82: pp. 1149-1156.
51. Colice G.L., Shafazand S., Griffin J.P., et. al.: Physiologic evaluation of the patient with lung cancer being considered for resectional surgery—ACCP evidenced-based clinical practice guidelines (2nd edition). Chest 2007; 132: pp. 161s-177s.
52. Kaushik S.S., Cleveland Z.I., Cofer G.P., et. al.: Diffusion-weighted hyperpolarized 129Xe MRI in healthy volunteers and subjects with chronic obstructive pulmonary disease. Magn Reson Med 2011; 65: pp. 1154-1165.
53. Wild J., Collier G., Marshall H., et. al.: P283 Hyperpolarised gas MRI—a pathway to clinical diagnostic imaging. Thorax 2015; 70: pp. A220-A221.
54. Johnson K.M., Fain S.B., Schiebler M.L., et. al.: Optimized 3D ultrashort echo time pulmonary MRI. Magn Reson Med 2013; 70: pp. 1241-1250.