
Rationale and Objectives
Concerns over medical radiation exposure have received national press in recent years, and training in the appropriate use of radiation has become an essential component of every radiology residency program. Appropriate training is particularly important in fluoroscopy because it is commonly used by inexperienced radiology residents and has the potential to impart relatively high patient radiation doses. In an effort to minimize the radiation doses received by patients, our institution has recently initiated an online training program in the safe use of fluoroscopy. This course is required and must be completed by new radiology residents before their first fluoroscopy rotation. The goal of this study was to determine if the use of an online course in the safe use of fluoroscopy could result in decreased patient dose without affecting diagnostic quality.
Materials and Methods
Four years of retrospective procedural data for residents performing gastrointestinal and genitourinary fluoroscopic procedures without specialized training were reviewed. Incoming residents took an American Medical Association–accredited online training program in the safe use of fluoroscopy the week before their first fluoroscopy rotation. Patient dose and diagnostic quality data, inferred from the frequency of attending physician intervention necessary to complete the procedure, were collected for all exams performed by the new group of residents after completion of the training course. This was then compared to data from prior classes and stratified by procedure type.
Results
Statistically significant reductions in both average fluoroscopy time (FT) or dose-area-product (DAP) were found for many of the fluoroscopic procedures performed by residents who participated in the online fluoroscopy training program. Specifically, statistically significant reductions in FT for barium enema, cystogram, defecogram, and esophagram procedures ( P < .001) were found. Esophagram and upper gastrointestinal studies were completed with a significantly lower DAP ( P < .001). The average reduction in DAP across all procedures performed by first-year residents was 38%, whereas the average reduction in FT was 25%. Based on a review of data from all procedures performed, there was no statistically significant loss in diagnostic quality.
Conclusion
An online training program can be effectively used to provide radiation safety instruction immediately before the start of a resident’s fluoroscopy rotation, decreasing patient dose without affecting diagnostic quality.
Fluoroscopy is an important imaging modality, because it allows for the real-time visualization of anatomic detail and function. This modality is widely used but imparts a relatively high radiation dose to the patient when compared to other diagnostic imaging modalities . As imaging techniques have become more widely used, medical imaging has led to a significant increase in cumulative radiation dose among the general population, with a corresponding potential increase in cancer risk . The National Council on Radiation Protection has reported a 5.7-fold increase in annual radiation dose from medical procedures in the United States between the early 1980s (effective dose of 0.53 mSv per individual from medical imaging) and 2006 (3.0 mSv per individual) . This increase is derived primarily from increasing use of computed tomography, nuclear medicine, and both interventional and conventional fluoroscopic procedures . In fact, fluoroscopic procedures such as upper gastrointestinal (GI) and barium enemas made up only 2.1% of all conventional radiography and fluoroscopy exams throughout the United States in 2007, but accounted for approximately 29.5% of the radiation dose associated with all such exams . Unlike other radiological imaging modalities, fluoroscopic procedures are performed directly by radiologists; for this reason, patient radiation doses are heavily influenced by physician technique .
Reducing patient radiation dose is a high priority in radiology residency programs. In addition to public concern regarding radiation effects, the increasing use of radiographic procedures makes it imperative that radiology residency programs teach safe fluoroscopic technique in order to reduce patient dose. Techniques for lowering patient dose include limiting the use of electronic and geometric magnification, collimating the beam to the area of interest, using pulsed fluoroscopy, keeping the patient as far from the x-ray source as possible, and keeping the image intensifier as close to the patient as possible . The drastic dose reduction associated with some of these techniques and their effect on image quality are not well understood by many residents. Specifically, many residents may be under the misconception that techniques that reduce dose may degrade image quality and increase the difficulty of diagnosis, when in fact the opposite is often true. Collimating to the area of interest and using pulsed fluoroscopy will both result in improved image quality, whereas other techniques provide dose reduction with no appreciable decrease in image quality when used appropriately . Proper resident training is essential for comprehension and correct implementation of these relatively complex concepts.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Number of Patient Studies Included Stratified by Study and Group with FT and DAP Data
Online ∗ PGY2 † Experienced ‡ Combined § FT (DAP) FT (DAP) FT (DAP) FT (DAP) Barium enema 77 (76) 45 (44) 151 (141) 196 (185) Cystogram 25 (25) 24 (23) 73 (73) 97 (96) Defecogram 25 (24) 33 (30) 97 (96) 130 (126) Esophagram 191 (189) 96 (95) 497 (496) 593 (591) Small bowel follow-through 34 (34) 39 (39) 148 (146) 187 (185) Upper GI 158 (156) 95 (89) 389 (386) 484 (475) Upper GI with small-bowel 11 (9) 14 (13) 63 (60) 77 (73) Voiding cystourethrogram 45 (43) 37 (37) 177 (176) 214 (213)
DAP, dose-area-product; FT, fluoroscopy time; GI, gastrointestinal; PGY2, postgraduate year 2.
Number of studies in which DAP is available is listed in parentheses; the number of available FT studies is listed without parentheses.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
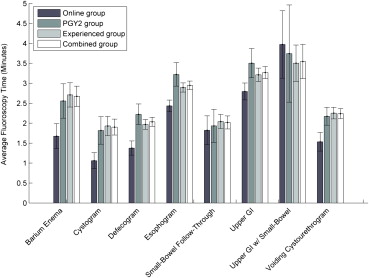
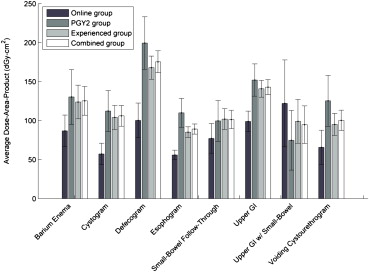
Table 2
Average Fluoroscopy Time in Minutes for Each Type of Study Performed, Stratified by Group
Online ∗ PGY2 † Experienced ‡ Combined § Barium enema 1.67 (1.42) 2.56 (1.48) || 2.71 (1.90) || 2.67 (1.81) || Cystogram 1.06 (0.51) 1.82 (0.86) || 1.93 (1.05) || 1.90 (1.00) || Defecogram 1.38 (0.45) 2.22 (0.76) || 1.97 (0.62) || 2.03 (0.67) || Esophagram 2.43 (1.03) 3.22 (1.47) || 2.89 (1.31) || 2.95 (1.34) || Small bowel follow-through 1.82 (1.08) 1.93 (1.32) 2.04 (1.10) 2.02 (1.14) Upper GI 2.80 (1.36) 3.50 (1.82) 3.21 (1.70) 3.27 (1.72) Upper GI with small bowel 3.97 (1.43) 3.74 (2.33) 3.50 (1.85) 3.55 (1.93) Voiding cystourethrogram 1.53 (0.80) 2.17 (0.70) 2.25 (0.99) || 2.24 (0.95) ||
GI, gastrointestinal; PGY2, postgraduate year 2.
Mean time per procedure is indicated with the standard deviation in parentheses.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Average DAP (dGy-cm 2 ) for Each Type of Study Performed, Stratified by Group
Online ∗ PGY2 † Experienced ‡ Combined § Barium enema 86.86 (90.52) 130.36 (118.97) 123.87 (130.78) 125.41 (127.78) Cystogram 57.32 (34.92) 112.39 (64.32) 104.15 (67.24) 106.12 (66.31) Defecogram 100.33 (55.68) 199.50 (94.24) || 167.96 (94.34) 175.47 (80.26) || Esophagram 56.00 (43.25) 110.08 (92.41) || 85.22 (78.16) || 89.21 (81.05) || Small bowel follow-through 77.24 (56.52) 99.67 (83.40) 101.98 (82.14) 101.49 (82.18) Upper GI 99.00 (84.29) 152.08 (99.57) || 140.80 (108.17) || 142.91 (106.60) || Upper GI with small bowel 122.16 (85.22) 74.85 (70.41) 99.17 (111.01) 94.84 (104.94) Voiding Cystourethrogram 65.81 (73.50) 125.41 (101.31) 95.13 (96.07) 100.39 (97.43)
DAP, dose-area-product; GI, gastrointestinal.
Mean DAP is indicated with the standard deviation in parentheses.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. European Society of Radiology (ESR): White paper on radiation protection by the European Society of Radiology. Insights Imaging 2011; 2: pp. 357-362.
2. Amis E.S., Butler P.F.: ACR white paper on radiation dose in medicine: three years later. J Am Coll Radiol 2010; 7: pp. 865-870.
3. Schauer D.A., Linton O.W.: National Council on Radiation Protection and Measurements report shows substantial medical exposure increase. Radiology 2009; 253: pp. 293-296.
4. National Council on Radiation Protection and Measurements: Ionizing radiation exposure of the population of the United States. National Council on Radiation Protection report no. 160.2009.National Council on Radiation Protection and MeasurementsBethesda, MD
5. Mahesh M.: Fluoroscopy: patient radiation exposure issues. Radiographics 2001; 21: pp. 1033-1045.
6. Wagner L.K., Archer B.R., Cohen A.M.: Management of patient skin dose in fluoroscopically guided interventional procedures. J Vasc Intervent Radiol 2000; 11: pp. 25-33.
7. Strauss K.: Pediatric interventional radiography equipment: safety considerations. Pediatr Radiol 2006; 36: pp. 126-135.
8. Jones AK, Pasciak AS, Steele J. A comprehensive course in the safe use of fluoroscopy, Fluoroscopic Safety, LLC. http://www.xraysafety.org . Accessed January 12, 2013.
9. Chang T, Medina J, Pirkle JK, et al. Fluoroscopy: an often overlooked source of radiation - The effect that level of training has on patient fluoroscopic radiation dosage, revisited. Poster session presented at: Annual Meeting of the Association of University Radiologists; 2012 March 19-22; San Antonio, TX.
10. Chenkin J., Lee S., Huynh T., et. al.: Procedures can be learned on the Web: a randomized study of ultrasound-guided vascular access training. Acad Emerg Med 2008; 15: pp. 949-954.
11. Lee J.M., Fernandez F., Staff I., Mah J.W.: Web-based teaching module improves success rates of postpyloric positioning of nasoenteric feeding tubes. JPEN J Parenter Enteral Nutr 2012; 36: pp. 323-329.
12. Beyea J.A., Wong E., Bromwich M., et. al.: Evaluation of a particle repositioning maneuver Web-based teaching module. Laryngoscope 2008; 118: pp. 175-180.
13. Schell S.R., Flynn T.C.: Web-based minimally invasive surgery training: competency assessment in PGY 1-2 surgical residents. Curr Surg 2004; 61: pp. 120-124.
14. Jones A.K., Pasciak A.S.: Calculating the peak skin dose resulting from fluoroscopically guided interventions. Part I: methods. J Appl Clin Med Phys 2011; 12: pp. 231-244.
15. Yu S.K., Cheung Y.K., Chan T.L., et. al.: Reduction of radiation dose to patients undergoing barium enema by dose audit. Br J Radiol 2001; 74: pp. 162-165.
16. American College of Radiology: ACR technical standard for management of the use of radiation in fluoroscopic procedures. Practice Guidelines and Technical Standards 2008.2008.American College of RadiologyReston, VApp. 1143-1149. http://www.acr.org/SecondaryMainMenuCategories/quality_safety/guidelines/med_phys/management_fluoro_procedures.aspx Accessed February 13, 2013
17. Texas Department of State Health Services. Use of radiation machines in the healing arts. Texas Administrative Code §289.227, 2013.