
Rationale and Objectives
The aims of this study were to determine the optimal image reconstruction intervals for the systolic and diastolic phases of coronary computed tomographic angiography on 256-slice computed tomography and to assess their associated motion artifacts.
Materials and Methods
One hundred twenty-six patients were recruited (mean heart rate [HR], 72.1 beats/min; heart rate variability, 1.3 beats/min). Twenty data sets were reconstructed in 5% steps through 0% to 95% of the R-R interval. Two reviewers discriminated optimal reconstruction intervals for 15 segments distributed in three coronary arteries on the basis of motion artifacts, which were graded from 1 (no motion artifacts) to 4 (severe motion artifacts preventing diagnosis). Patients were then stratified into four HR groups for motion score comparison according to the results of a correlation analysis of HR and motion scores.
Results
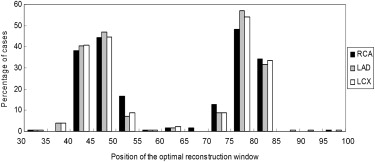
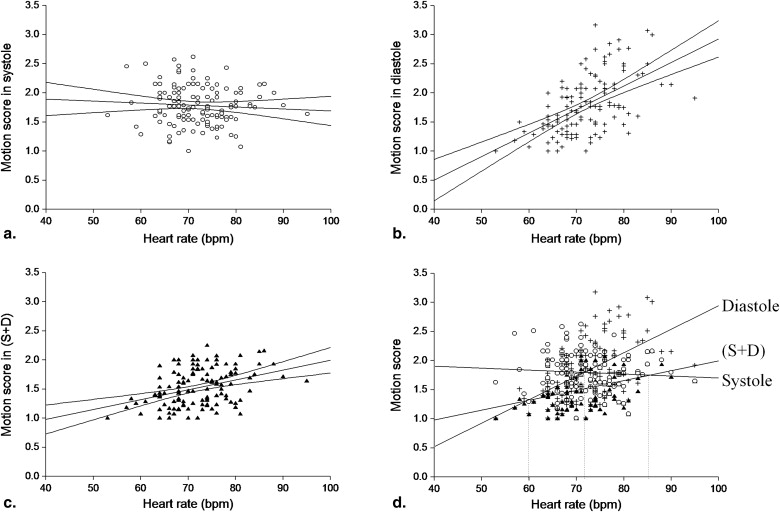
The optimal systolic and diastolic reconstruction intervals were 44.4 ± 3.8% and 77.4 ± 3.7%, respectively. The mean motion scores for systolic, diastolic, and combined systolic and diastolic (S+D) reconstructions were 1.8 ± 0.3, 1.8 ± 0.5, and 1.5 ± 0.3, respectively. Combined S+D reconstruction improved diagnostic evaluability to 100% and showed fewer motion artifacts compared to single-phase reconstructions for all HR ranges (S+D vs systolic, P < .05 for HR < 85 beats/min; S+D vs diastolic, P < .05 for HRs of 73–84 beats/min). For HRs of 60 to 72 beats/min, motion artifacts were significantly lower for diastole (1.6 ± 0.3) than systole (1.8 ± 0.4) ( P < .001), and vice versa for HRs of 73 to 84 beats/min (1.7 ± 0.3 for systole vs 2.0 ± 0.5 for diastole, P < .01).
Conclusions
Optimal systolic and diastolic reconstruction intervals were determined for this 256-slice coronary computed tomographic angiographic study. Combined reconstruction showed fewer motion artifacts compared to single-phase reconstruction. In conclusion, 256-slice computed tomography has the potential to improve the diagnostic accuracy of coronary computed tomographic angiography.
Multidetector computed tomographic (CT) imaging continues to evolve as a powerful diagnostic tool for the noninvasive imaging of coronary artery disease . Both 64-slice and dual-source CT imaging enhance coronary CT angiography for patients within certain ranges of mean heart rate (HR) and HR variability (HRV) . However, because of constant cardiac motion and the short quiescent phase of the cardiac cycle, especially in patients with high HRs, multidetector CT technology with high temporal resolution and short acquisition time is essential to image the coronary arteries without substantial motion artifacts.
The recently introduced 256-slice CT technology offers superior temporal resolution, with a minimum of 135 ms, compared to 210 ms for 64-slice CT systems . Additionally, these scanners provides z -axis coverage of 80 mm, allowing an acquisition time for the whole heart as low as 5 seconds for 120-mm z -axis coverage . The currently reported scan time for single-source and dual-source 64-slice coronary CT angiography is on the order of 6 to 10 seconds .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patient Population
Get Radiology Tree app to read full this article<
Table 1
Demographic Data of Patients
Variable Value Number of patients 126 Age (y) 56.5 ± 9.8 Women/men 49/77 Body mass index (kg/m 2 ) 25.6 ± 4.0 Heart rate range (beats/min) 53–95 Heart rate (beats/min) 72.1 ± 6.9 Heart rate variability (beats/min) 1.3 ± 0.7 Tube voltage (kV) 120.2 ± 1.8 Tube current (mA) 565.7 ± 91.7 Tube rotation time (ms) 0.27 ± 0.00 Scan time (s) 4.9 ± 0.3 Scan length (mm) 129.7 ± 13.8
Data are expressed as number, as mean ± standard deviation, or as range.
Get Radiology Tree app to read full this article<
CT Acquisition Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Data Postprocessing and Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Motion Artifacts of Coronary Artery Segments in Their Optimal Systolic Reconstruction Interval
Get Radiology Tree app to read full this article<
Table 2
Optimal Reconstruction Interval, Motion Score, Its Correlation with Mean Heart Rate and Heart Rate Variability: Systolic Phase
Variable Total RCA LAD LCX Optimal systolic reconstruction (%) 44.4 ± 3.8 45.1 ± 3.8 44.0 ± 3.8 44.0 ± 3.8 Median systolic reconstruction (%) 45 45 45 45 Overall image quality score 1.8 ± 0.3 1.8 ± 0.5 1.7 ± 0.4 1.9 ± 0.5 1 31.5% (519/1649 ∗ ) 32.6% (159/488) 36.1% (249/690) 24.2% (104/429) 2 58.4% (963/1649) 53.9% (263/488) 57.1% (394/690) 63.4% (272/429) 3 10.1% (167/1649) 13.5% (66/488) 6.8% (47/690) 12.4% (53/429) 4 0.0 (0/1649) 0.0 (0/488) 0.0 (0/690) 0.0 (0/429) Correlation ( r ) with mean heart rate ( P ) −0.07 (.44) 0.01 (.89) −0.09 (.32) −0.07 (.46) Correlation ( r ) with heart rate variability ( P ) 0.01 (.99) −0.07 (.47) 0.08 (.35) −0.03 (.75)
The right coronary artery (RCA) includes segments 1 to 4, the left anterior descending coronary artery (LAD) includes segments 5 to 10, and the left circumflex coronary artery (LCX) includes segments 11 to 15.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Motion Artifacts of Coronary Artery Segments in Their Optimal Diastolic Reconstruction Interval
Get Radiology Tree app to read full this article<
Table 3
Optimal Reconstruction Interval, Motion Score, Its Correlation with Mean Heart Rate and Heart Rate Variability: Diastolic Phase
Variable Total RCA LAD LCX Optimal diastolic reconstruction (%) 77.4 ± 3.7 77.1 ± 4.4 77.4 ± 3.4 77.7 ± 3.5 Median diastolic reconstruction (%) 78 78 78 78 Overall image quality score 1.8 ± 0.5 2.0 ± 0.7 1.7 ± 0.5 1.8 ± 0.6 1 37.0% (610/1649 ∗ ) 28.3% (138/488) 44.6% (308/690) 34.3% (147/429) 2 48.6% (801/1649) 45.7% (223/488) 45.4% (313/690) 56.4% (242/429) 3 12.8% (211/1649) 21.5% (105/488) 9.4% (65/690) 9.1% (39/429) 4 1.6% (26/1649) 4.3% (21/488) 0.6% (4/690) 0.2% (1/429) Correlation ( r ) with mean heart rate ( P ) 0.55 (<.001) 0.55 (<.001) 0.42 (<.0001) 0.51 (<.001) Correlation ( r ) with heart rate variability ( P ) −0.09 (.32) −0.11 (.21) −0.06 (.51) −0.06 (.51)
The right coronary artery (RCA) includes segments 1 to 4, the left anterior descending coronary artery (LAD) includes segments 5 to 10, and the left circumflex coronary artery (LCX) includes segments 11 to 15.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Motion Artifacts of Coronary Artery Segments in the Combined Reconstruction Interval
Get Radiology Tree app to read full this article<
Table 4
Motion Score and Its Correlation with Mean Heart Rate and Heart Rate Variability: Combined Systolic and Diastolic Phase
Total RCA LAD LCX Overall image quality score 1.5 ± 0.3 1.6 ± 0.4 1.4 ± 0.3 1.6 ± 0.4 1 50.6% (835/1649 ∗ ) 44.3% (216/488) 58.4% (403/690) 45.7% (196/429) 2 46.8% (771/1649) 49.8% (243/488) 40.4% (279/690) 52.9% (227/429) 3 2.6% (43/1649) 5.9% (29/488) 1.2% (8/690) 1.4% (6/429) 4 0.0% (0/1649) 0.0% (0/488) 0.0% (0/690) 0.0% (0/429) Correlation ( r ) with mean heart rate ( P ) 0.37 (<.0001) 0.29 (<.01) 0.27 (<.01) 0.39 (<.00001) Correlation ( r ) with heart rate variability ( P ) −0.07 (.43) −0.07 (.43) −0.07 (.44) −0.02 (.82)
The right coronary artery (RCA) includes segments 1 to 4, the left anterior descending coronary artery (LAD) includes segments 5 to 10, and the left circumflex coronary artery (LCX) includes segments 11 to 15.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Motion Artifact Comparison for Different HR Ranges
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Marano R., De Cobelli F., Floriani I., et. al.: Italian multicenter, prospective study to evaluate the negative predictive value of 16-and 64-slice MDCT imaging in patients scheduled for coronary angiography (NIMISCAD-Non Invasive Multicenter Italian Study for Coronary Artery Disease). Eur Radiol 2009; 19: pp. 1114-1123.
2. Herzka D.A., Gharib A.M.: Should all patients with suspected coronary artery disease undergo coronary angiography with 16-row MDCT?. Nat Clin Pract Cardiovasc Med 2007; 4: pp. 74-75.
3. Nikolaou K., Rist C., Wintersperger B.J., et. al.: Clinical value of MDCT in the diagnosis of coronary artery disease in patients with a low pretest likelihood of significant disease. AJR Am J Roentgenol 2006; 186: pp. 1659-1668.
4. Johnson T.R., Nikolaou K., Wintersperger B.J., et. al.: Dual-source CT cardiac imaging: initial experience. Eur Radiol 2006; 16: pp. 1409-1415.
5. Rist C., Johnson T.R., Becker A., et. al.: Dual-source cardiac CT imaging with improved temporal resolution. Impact on image quality and analysis of left ventricular function [article in German]. Radiologe 2007; 47: pp. 287-290. 292–294
6. Rogalla P., Kloeters C., Hein P.A.: CT technology overview: 64-slice and beyond. Radiol Clin North Am 2009; 47: pp. 1-11.
7. Stein P.D., Yaekoub A.Y., Matta F., Sostman H.D.: 64-slice CT for diagnosis of coronary artery disease: a systematic review. Am J Med 2008; 121: pp. 715-725.
8. Matt D., Scheffel H., Leschka S., et. al.: Dual-source CT coronary angiography: image quality, mean heart rate, and heart rate variability. AJR Am J Roentgenol 2007; 189: pp. 567-573.
9. Leschka S., Stolzmann P., Schmid F.T., et. al.: Low kilovoltage cardiac dual-source CT: attenuation, noise, and radiation dose. Eur Radiol 2008; 18: pp. 1809-1817.
10. Klass O., Walker M., Siebach A., et. al.: Prospectively gated axial CT coronary angiography: comparison of image quality and effective radiation dose between 64- and 256-slice CT. Eur Radiol 2010; 20: pp. 1124-1131.
11. Jakobs T.F., Becker C.R., Ohnesorge B., et. al.: Multislice helical CT of the heart with retrospective ECG gating: reduction of radiation exposure by ECG-controlled tube current modulation. Eur Radiol 2002; 12: pp. 1081-1086.
12. Haraldsdottir S, Gudnason T, Sigurdsson AF, et al. Diagnostic accuracy of 64-slice multidetector CT for detection of in-stent restenosis in an unselected, consecutive patient population. Eur J Radiol. In press.
13. Ertel D., Lell M.M., Harig F., Flohr T., Schmidt B., Kalender W.A.: Cardiac spiral dual-source CT with high pitch: a feasibility study. Eur Radiol 2009; 19: pp. 2357-2362.
14. Leschka S., Husmann L., Desbiolles L.M., et. al.: Optimal image reconstruction intervals for non-invasive coronary angiography with 64-slice CT. Eur Radiol 2006; 16: pp. 1964-1972.
15. Seifarth H., Wienbeck S., Püsken M., et. al.: Optimal systolic and diastolic reconstruction windows for coronary CT angiography using dual-source CT. AJR Am J Roentgenol 2007; 189: pp. 1317-1323.
16. Sanz J., Rius T., Kuschnir P., et. al.: The importance of end-systole for optimal reconstruction protocol of coronary angiography with 16-slice multidetector computed tomography. Invest Radiol 2005; 40: pp. 155-163.
17. Wintersperger B.J., Nikolaou K., von Ziegler F., et. al.: Image quality, motion artifacts, and reconstruction timing of 64-slice coronary computed tomography angiography with 0.33-second rotation speed. Invest Radiol 2006; 41: pp. 436-442.
18. Hausleiter J., Meyer T., Hadamitzky M., et. al.: Radiation dose estimates from cardiac multislice computed tomography in daily practice: impact of different scanning protocols on effective dose estimates. Circulation 2006; 113: pp. 1305-1310.
19. Earls J.P., Berman E.L., Urban B.A., et. al.: Prospectively gated transverse coronary CT angiography versus retrospectively gated helical technique: improved image quality and reduced radiation dose. Radiology 2008; 246: pp. 742-753.
20. Hirai N., Horiguchi J., Fujioka C., et. al.: Prospective versus retrospective ECG-gated 64-detector coronary CT angiography: assessment of image quality, stenosis, and radiation dose. Radiology 2008; 248: pp. 424-430.
21. Shuman W.P., Branch K.R., May J.M., et. al.: Prospective versus retrospective ECG gating for 64-detector CT of the coronary arteries: comparison of image quality and patient radiation dose. Radiology 2008; 248: pp. 431-437.
22. Ohnesorge B., Becker C.R., Flohr T., Reiser M.F.: Multi-slice CT in Cardiac Imaging.2002.SpringerNew York
23. Cademartiri F., Nieman K., van der Lugt A., et. al.: Intravenous contrast material administration at 16-detector row helical CT coronary angiography: test bolus versus bolus-tracking technique. Radiology 2004; 233: pp. 817-823.
24. Kachelriess M., Ulzheimer S., Kalender W.A.: ECG-correlated image reconstruction from subsecond multi-slice spiral CT scans of the heart. Med Phys 2000; 27: pp. 1881-1902.
25. Flohr T., Ohnesorge B.: Heart rate adaptive optimization of spatial and temporal resolution for electrocardiogram-gated multislice spiral CT of the heart. J Comput Assist Tomogr 2001; 25: pp. 907-923.
26. Austen W.G., Edwards J.E., Frye R.L., et. al.: A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 1975; 51: pp. 5-40.
27. Leschka S., Wildermuth S., Boehm T., et. al.: Noninvasive coronary angiography with 64-section CT: effect of average heart rate and heart rate variability on image quality. Radiology 2006; 241: pp. 378-385.
28. Choi H.S., Choi B.W., Choe K.O., et. al.: Pitfalls, artifacts, and remedies in multi-detector row CT coronary angiography. Radiographics 2004; 24: pp. 787-800.
29. Hu H.: Multi-slice helical CT: scan and reconstruction. Med Phys 1999; 26: pp. 5-18.
30. Taguchi K., Aradate H.: Algorithm for image reconstruction in multi-slice helical CT. Med Phys 1998; 25: pp. 550-561.
31. Prat-Gonzalez S., Sanz J., Garcia M.J.: Cardiac CT: indications and limitations. J Nucl Med Technol 2008; 36: pp. 18-24.
32. Seifarth H., Puesken M., Wienbeck S., et. al.: Automatic selection of optimal systolic and diastolic reconstruction windows for dual-source CT coronary angiography. Eur Radiol 2009; 19: pp. 1645-1652.
33. Poll L.W., Cohnen M., Brachten S., Ewen K., Mödder U.: Dose reduction in multi-slice CT of the heart by use of ECG-controlled tube current modulation (“ECG pulsing”): phantom measurements. Rofo 2002; 174: pp. 1500-1505.
34. Bley T.A., Ghanem N.A., Foell D., et. al.: Computed tomography coronary angiography with 370-millisecond gantry rotation time—evaluation of the best image reconstruction interval. J Comput Assist Tomogr 2005; 29: pp. 1-5.
35. Herzog C., Arning-Erb M., Zangos S., et. al.: Multi-detector row CT coronary angiography: influence of reconstruction technique and heart rate on image quality. Radiology 2006; 238: pp. 75-86.