
Rationale and Objectives
Dual-energy computed tomography (DECT) offers various fields of application, especially in angiography using virtual monoenergetic imaging. The aim of this study was to evaluate objective image quality indices of calculated low–kiloelectron volt monoenergetic DECT angiographic cervical and cerebral data sets compared to virtual 120-kV polyenergetic images.
Materials and Methods
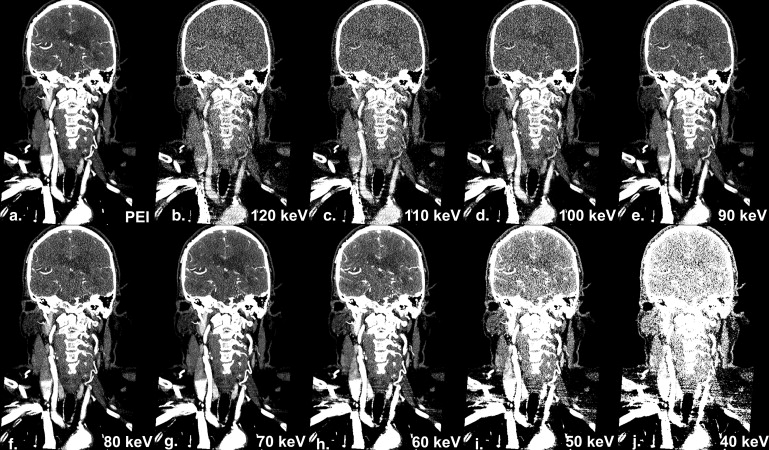
Forty-one patients (21 men, mean age 58 ± 14) who underwent DECT angiography of the cervical ( n = 7) or cerebral vessels ( n = 34) were retrospectively included in this study. Data acquired with the 80 and 140 kVp tube using dual-source CT technology were subsequently used to calculate low-kiloelectron volt monoenergetic image data sets ranging from 120 to 40 keV (at 10-keV intervals per patient). Vessel and soft tissue attenuation and image noise were measured in various regions of interest, and contrast-to-noise ratio (CNR) was subsequently calculated. Differences in image attenuation and CNR were compared between the different monoenergetic data sets and virtual 120-kV polyenergetic images.
Results
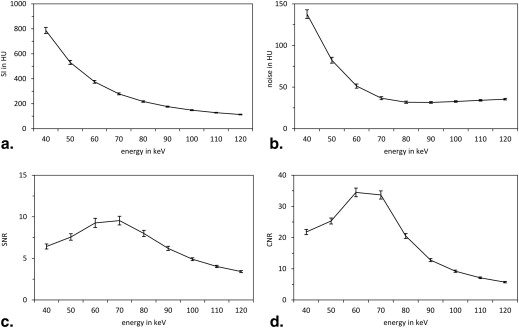
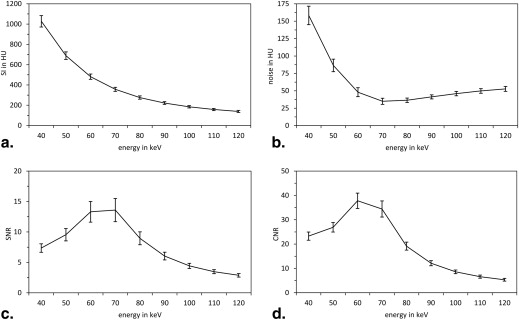
For cervical angiography, 60-keV monoenergetic data sets resulted in the greatest improvements in vessel attenuation and CNR compared to virtual 120-kV polyenergetic data sets (+40%, +16%; all P < .01). Also for cerebral vessel assessment, 60-keV monoenergetic data sets provided the greatest improvement in vessel attenuation and CNR (+40%, +9%; all P < .01) compared to virtual 120-kV polyenergetic data sets.
Conclusions
60-keV monoenergetic image data significantly improve vessel attenuation and CNR of cervical and cerebral DECT angiographic studies. Future studies have to evaluate whether the technique can lead to an increased diagnostic accuracy or should be used for dose reduction of iodinated contrast material.
The clinical and experimental applications of dual-energy computed tomography (DECT) imaging continue to expand. DECT acquires data sets at two different energy levels and uses the differential x-ray absorption characteristics of different materials to identify and map various components within an image. This includes urate crystals, calcium, and iodine. Accordingly, DECT techniques have been used in a range of scenarios, including tissue perfusion analysis in cardiology and oncology, gout imaging, renal cyst characterization, and bone/calcified atherosclerotic plaque subtraction . DECT has been specifically applied in head and neck CT angiography for bone and plaque removal to improve the accuracy of intracranial hemorrhage detection and to identify the underlying etiology of intracranial hematomas .
DECT may also have a role in improving the image quality of head and neck CT angiography. In most cases, a 120-kVp single-energy equivalent series is reconstructed from the two DECT data sets. Like standard single-energy CT, these images are created from a polyenergetic x-ray spectrum with the peak energy represented by the kVp. It is possible, however, to use DECT basis material decomposition and the knowledge of specific linear attenuation coefficients to calculate the expected mass attenuation coefficient for each voxel at any energy level, resulting in “virtual monoenergetic” images (MEIs). Considering the impact of tube energy settings on radiation dose, noise, attenuation, and overall image quality, this added DECT-based functionality might provide several advantages compared to the traditional reconstructions. Contrast-enhanced vessel attenuation increases with decreasing x-ray energies (down to the K-edge of iodine, 33 keV) . It has been shown that lower energy acquisitions can lead to better image quality and reduction of contrast material administration . Similar results were found in CT pulmonary angiographic studies using DECT, in which low-kiloelectron volt MEIs allowed iodine load reduction while improving vascular attenuation and maintaining signal-to-noise ratios (SNR) compared to single-energy CT .
Get Radiology Tree app to read full this article<
Materials and methods
Study Population
Get Radiology Tree app to read full this article<
Image Acquisitions
Get Radiology Tree app to read full this article<
Image Reconstruction
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
SNR=attenuationvessel/noisevessel SNR
=
attenuation
vessel
/
noise
vessel
CNR=(attenuationvessel−attenuationmuscle)/noiseair. CNR
=
(
attenuation
vessel
−
attenuation
muscle
)
/
noise
air
.
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Cerebral Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Relative Comparison of Objective Image Quality Parameters between 70- and 60-keV MEI Versus 120-kV PEI in DECT Angiography of Cervical and Cerebral Vessels
70-keV Versus 120-kV PEI (%)P Value 60-keV Versus 120-kV PEI (%)P Value Attenuation Cervical +3 <.01 +40 <.01 Cerebral +3 <.01 +40 <.01 Noise Cervical 0 +39 <.01 Cerebral +3 <.01 +50 <.01 SNR Cervical 0 +8 <.49 Cerebral 0 0 CNR Cervical +3 <.01 +16 <.01 Cerebral +9 <.01 +9 <.01
CNR, contrast-to-noise ratio; DECT, dual-energy computed tomography; MEI, monoenergetic image; PEI, polyenergetic image; SNR, signal-to-noise ratio.
Averaged above all investigated arteries per protocol. Shapiro–Wilk test was performed to estimate data distribution. For normal distributed data, two-sided Student t -Test and for non-normal distributed data, Wilcoxon signed-rank test were used. P < .05 was regarded significant.
Get Radiology Tree app to read full this article<
Cervical Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. McQueen F.M., Reeves Q., Dalbeth N.: New insights into an old disease: advanced imaging in the diagnosis and management of gout. Postgrad Med J 2012; 89: pp. 87-93.
2. Vliegenthart R., Pelgrim G.J., Ebersberger U., et. al.: Dual-energy CT of the heart. AJR Am J Roentgenol 2012; 199: pp. S54-S63.
3. Johnson T., Fink C., Schönberg S.O., et. al.: Dual energy CT in clinical practice.2011.SpringerBerlin Heidelberg
4. Weininger M., Schoepf U.J., Ramachandra A., et. al.: Adenosine-stress dynamic real-time myocardial perfusion CT and adenosine-stress first-pass dual-energy myocardial perfusion CT for the assessment of acute chest pain: initial results. Eur J Radiol 2012; 81: pp. 3703-3710.
5. Meyer M., Hohenberger P., Apfaltrer P., et. al.: CT-based response assessment of advanced gastrointestinal stromal tumor: dual energy CT provides a more predictive imaging biomarker of clinical benefit than RECIST or Choi criteria. Eur J Radiol 2013; 82: pp. 923-928.
6. Korn A., Bender B., Thomas C., et. al.: Dual energy CTA of the carotid bifurcation: advantage of plaque subtraction for assessment of grade of the stenosis and morphology. Eur J Radiol 2011; 80: pp. e120-e125.
7. Werncke T., Albrecht T., Wolf K.J., et. al.: Dual energy CT of the peripheral arteries: a phantom study to assess the effect of automatic plaque removal on stenosis grading. Rofo 2010; 182: pp. 682-689.
8. Postma A.A., Hofman P.A., Stadler A.A., et. al.: Dual-energy CT of the brain and intracranial vessels. AJR Am J Roentgenol 2012; 199: pp. S26-S33.
9. Vlahos I., Godoy M.C., Naidich D.P.: Dual-energy computed tomography imaging of the aorta. J Thorac Imaging 2010; 25: pp. 289-300.
10. Kim M.J., Park C.H., Choi S.J., et. al.: Multidetector computed tomography chest examinations with low-kilovoltage protocols in adults: effect on image quality and radiation dose. J Comput Assist Tomogr 2009; 33: pp. 416-421.
11. Matsuoka S., Hunsaker A.R., Gill R.R., et. al.: Vascular enhancement and image quality of MDCT pulmonary angiography in 400 cases: comparison of standard and low kilovoltage settings. AJR Am J Roentgenol 2009; 192: pp. 1651-1656.
12. Nakayama Y., Awai K., Funama Y., et. al.: Lower tube voltage reduces contrast material and radiation doses on 16-MDCT aortography. AJR Am J Roentgenol 2006; 187: pp. W490-W497.
13. Schueller-Weidekamm C., Schaefer-Prokop C.M., Weber M., et. al.: CT angiography of pulmonary arteries to detect pulmonary embolism: improvement of vascular enhancement with low kilovoltage settings. Radiology 2006; 241: pp. 899-907.
14. Szucs-Farkas Z., Kurmann L., Strautz T., et. al.: Patient exposure and image quality of low-dose pulmonary computed tomography angiography: comparison of 100- and 80-kVp protocols. Invest Radiol 2008; 43: pp. 871-876.
15. Godoy M.C., Heller S.L., Naidich D.P., et. al.: Dual-energy MDCT: comparison of pulmonary artery enhancement on dedicated CT pulmonary angiography, routine and low contrast volume studies. Eur J Radiol 2011; 79: pp. e11-e17.
16. Yuan R., Shuman W.P., Earls J.P., et. al.: Reduced iodine load at CT pulmonary angiography with dual-energy monochromatic imaging: comparison with standard CT pulmonary angiography–a prospective randomized trial. Radiology 2012; 262: pp. 290-297.
17. Yu L., Christner J.A., Leng S., et. al.: Virtual monochromatic imaging in dual-source dual-energy CT: radiation dose and image quality. Med Phys 2011; 38: pp. 6371-6379.
18. Okayama S., Seno A., Soeda T., et. al.: Optimization of energy level for coronary angiography with dual-energy and dual-source computed tomography. Int J Cardiovasc Imaging 2012; 28: pp. 901-909.
19. Bamberg F., Dierks A., Nikolaou K., et. al.: Metal artifact reduction by dual energy computed tomography using monoenergetic extrapolation. Eur Radiol 2011; 21: pp. 1424-1429.
20. Behrendt F.F., Schmidt B., Plumhans C., et. al.: Image fusion in dual energy computed tomography: effect on contrast enhancement, signal-to-noise ratio and image quality in computed tomography angiography. Invest Radiol 2009; 44: pp. 1-6.