
Rationale and Objectives
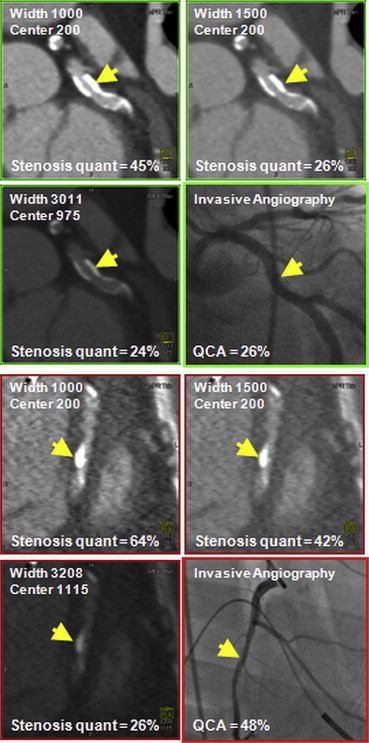
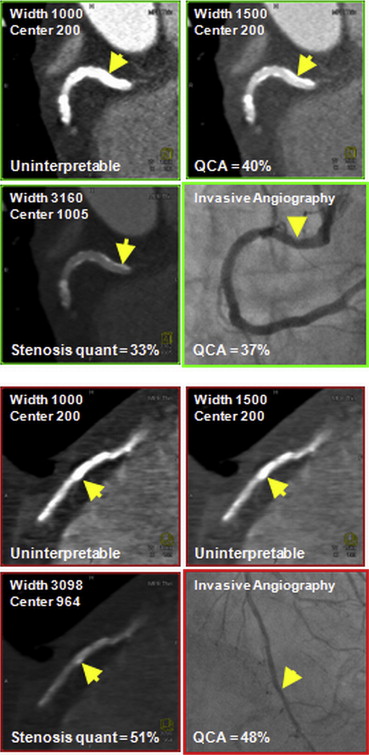
Blooming artifact from calcified plaques often renders measurement of stenosis impossible on coronary computed tomographic angiography (CTA). We sought to evaluate the impact of modifying window level on reducing blooming artifact, and its impact on stenosis quantification.
Materials and Methods
We analyzed 125 calcified segments from 53 patients who underwent CTA and invasive coronary angiography (ICA). Segmental stenosis on CTA was measured using three window settings: width of 1000 Hounsfield units (HU) and level of 200 HU (“default”), 1500/200 HU (“widened”), and width and level based on the mean HU of the calcified plaque and pericoronary fat (“calcium-specific”). Segmental stenosis on ICA was quantified by a blinded experienced reader.
Results
ICA found ≥50% stenosis in 30 segments. Displaying segments with widened and calcium-specific settings improved overall accuracy of detecting ≥50% stenosis ( P ‘s < 0.001) by increasing the rate of accurately quantifying <50% stenosis ( P ‘s < 0.001), and improved correlation of stenosis quantification to ICA ( P ‘s < 0.05). There was no difference in stenosis quantification accuracy between widened and calcium-specific window settings. Limits of agreement between CTA stenosis quantification and ICA narrowed with widened and calcium-specific settings.
Conclusions
We showed for the first time that in calcified segments, widening display window width significantly improved CTA quantification of stenosis compared to ICA.
From the time of the introduction of coronary computed tomographic angiography (CTA) as a diagnostic tool, multiple studies have shown degradation in the accuracy of CTA when coronary arteries contain heavy calcification, resulting in significant reductions in both sensitivity and specificity . Calcification causes “blooming” artifact, which produces a falsely enlarged appearance of the plaque from partial-volume averaging effects . Blooming can be severe enough to render segments uninterpretable . Such difficulty has prompted some investigators to advise against performance of CTA when prior imaging has already documented a high coronary calcium score (CCS) .
When interpreting CTA image, the apparent size of calcification can be reduced by increasing display window width, potentially reducing blooming artifact. However, its impact on stenosis evaluation has not been investigated. We evaluated whether increasing the window width improved stenosis quantification of calcified coronary artery segments on CTA compared to invasive coronary angiography (ICA).
Materials and methods
Study Population
Get Radiology Tree app to read full this article<
Coronary Calcium Scoring
Get Radiology Tree app to read full this article<
CTA Performance and Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ICA Performance and Evaluation
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Characteristics of Patients and Coronary Artery Segments
Count (%) or Mean ± SD Median (Range)Patient characteristics: n = 53 Age 70 ± 9 71 (44–87) Men 32 (60) — BMI 26.7 ± 4.1 26.4 (18.9–35.5) Diabetes 16 (30) — Hypercholesterolemia 40 (75) — Hypertension 33 (65) — Currently smoking 5 (9) — Family CAD history 16 (30) — Asymptomatic 12 (23) — Typical angina 12 (23) — Total Agatston score 1309 ± 807 1160 (224–3255) Peak heart rate during CTA 70 ± 22 65 (44–187) Heart rate variation during CTA 11 ± 21 5 (0–134)Segment characteristics: n = 125 Left main 13 (10) — Left anterior descending 53 (42) — Circumflex 19 (15) — Right coronary 40 (32) — Agatston score of qualifying plaque 259 ± 210 187 (101–1027) Volume score of qualifying plaque 201 ± 159 154 (72–747) Calcium >180° arc at stenotic site 46 (37) — Multiple calcifications at stenosis 31 (25) — ≥50% Diameter stenosis by QCA 30 (24) —
BMI, body mass index; CAD, coronary artery disease; CTA, coronary computed tomographic angiography; QCA, quantitative coronary angiography; SD, standard deviation.
Get Radiology Tree app to read full this article<
Evaluable Segments: Reader 1
Get Radiology Tree app to read full this article<
Table 2
Performance of CTA Quantification Accuracy Using Different Window Settings in Evaluable Segment
Default (D) Widened (W) Calcium-specific (CS) Comparison P values W to D CS to D CS to W Reader 1 ( n = 113) With ≥50% stenosis on QCA 27 27 27 — — — Correctly found by CTA quantification 23/27 (85%) 22/27 (81%) 20/27 (74%) .596 .193 .407 With <50% stenosis on QCA 86 86 86 — — — Correctly found by CTA quantification 51/86 (59%) 72/86 (84%) 77/86 (90%) <.001 <.001 .096 CTA PPV 23/58 (40%) 22/36 (61%) 20/29 (70%) .043 .010 .510 CTA NPV 51/55 (93%) 72/77 (94%) 77/84 (92%) .861 .821 .657 Total accuracy by CTA 74/113 (65%) 94/113 (83%) 97/113 (86%) <.001 <.001 .394 CTA quantification within 10% of QCA 45/113 (40%) 66/113 (58%) 67/113 (59%) <.001 <.001 .846 Spearman correlation 0.53 0.63 0.64 .005 .012 .379 Reader 2 ( n = 117) With ≥50% stenosis on QCA 27 27 27 — — — Correctly found by CTA quantification 15/27 (56%) 13/27 (48%) 13/27 (48%) .435 .435 1.000 With <50% stenosis on QCA 90 90 90 — — — Correctly found by CTA quantification 62/90 (69%) 81/90 (90%) 82/90 (91%) <.001 <.001 .714 CTA PPV 15/33 (45%) 13/22 (59%) 13/21 (62%) .322 .238 .850 CTA NPV 62/74 (84%) 81/95 (85%) 82/96 (85%) .791 .769 .976 Total accuracy by CTA 77/117 (66%) 94/117 (80%) 95/117 (81%) <.001 <.001 .803 CTA quantification within 10% of QCA 43/117 (37%) 50/117 (43%) 53/117 (45%) .190 .063 .578 Spearman correlation 0.36 0.44 0.47 .028 .011 .101
CTA, coronary computed tomographic angiography; NPV, negative predictive value; PPV, positive predictive value; QCA, quantitative coronary angiography.
Table 3
Results of Bland–Altman Analysis of Agreement between CTA and QCA Using Different Window Settings
n Mean Difference (%) Lower Limit of Agreement (%) Upper Limit of Agreement (%) Range of Agreement Limits (%) Reader 1 Default 113 8.7 −25.0 42.4 67.4 Widened 113 0.5 −28.9 29.9 59.7 Calcium-specific 113 −1.5 −29.4 26.4 56.0 Reader 2 Default 117 4.6 −30.4 39.6 70.0 Widened 117 −5.7 −40.3 28.9 69.2 Calcium-specific 117 −7.4 −42.3 27.5 69.8
CTA, coronary computed tomographic angiography; QCA, quantitative coronary angiography.
Get Radiology Tree app to read full this article<
Evaluable Segments: Reader 2
Get Radiology Tree app to read full this article<
Uninterpretable Segments: Reader 1
Get Radiology Tree app to read full this article<
Uninterpretable Segments: Reader 2
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Potential Predictors of Improvement with Widened and Calcium-specific Window Settings
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Meijs M.F., Meijboom W.B., Prokop M., et. al.: Is there a role for CT coronary angiography in patients with symptomatic angina? Effect of coronary calcium score on identification of stenosis. Int J Cardiovasc Imaging 2009; 25: pp. 847-854.
2. Meng L., Cui L., Cheng Y., et. al.: Effect of heart rate and coronary calcification on the diagnostic accuracy of the dual-source CT coronary angiography in patients with suspected coronary artery disease. Korean J Radiol 2009; 10: pp. 347-354.
3. Zhang S., Levin D.C., Halpern E.J., et. al.: Accuracy of MDCT in assessing the degree of stenosis caused by calcified coronary artery plaques. AJR Am J Roentgenol 2008; 191: pp. 1676-1683.
4. Husmann L., Gaemperli O., Schepis T., et. al.: Accuracy of quantitative coronary angiography with computed tomography and its dependency on plaque composition: plaque composition and accuracy of cardiac CT. Int J Cardiovasc Imaging 2008; 24: pp. 895-904.
5. Raff G.L., Gallagher M.J., O’Neill W.W., et. al.: Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 2005; 46: pp. 552-557.
6. Hoffmann U., Ferencik M., Cury R.C., et. al.: Coronary CT angiography. J Nucl Med 2006; 47: pp. 797-806.
7. Stolzmann P., Scheffel H., Leschka S., et. al.: Influence of calcifications on diagnostic accuracy of coronary CT angiography using prospective ECG triggering. AJR Am J Roentgenol 2008; 191: pp. 1684-1689.
8. Kuettner A., Trabold T., Schroeder S., et. al.: Noninvasive detection of coronary lesions using 16-detector multislice spiral computed tomography technology: initial clinical results. J Am Coll Cardiol 2004; 44: pp. 1230-1237.
9. Taylor A.J., Cerqueira M., Hodgson J.M., et. al.: ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. J Cardiovasc Comput Tomogr 2010; 4: pp. 407.e1-407.e33.
10. Diederichsen A.C., Petersen H., Jensen L.O., et. al.: Diagnostic value of cardiac 64-slice computed tomography: importance of coronary calcium. Scand Cardiovasc J 2009; 43: pp. 337-344.
11. Agatston A.S., Janowitz W.R., Hildner F.J., et. al.: Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990; 15: pp. 827-832.
12. Gutstein A., Dey D., Cheng V., et. al.: Algorithm for radiation dose reduction with helical dual source coronary computed tomography angiography in clinical practice. J Cardiovasc Comput Tomogr 2008; 2: pp. 311-322.
13. Budoff M.J., Cohen M.C., Garcia M.J., et. al.: ACCF/AHA clinical competence statement on cardiac imaging with computed tomography and magnetic resonance. Circulation 2005; 112: pp. 598-617.
14. Ferencik M., Ropers D., Abbara S., et. al.: Diagnostic accuracy of image postprocessing methods for the detection of coronary artery stenoses by using multidetector CT. Radiology 2007; 243: pp. 696-702.
15. Ropers D., Baum U., Pohle K., et. al.: Detection of coronary artery stenoses with thin-slice multi-detector row spiral computed tomography and multiplanar reconstruction. Circulation 2003; 107: pp. 664-666.
16. Cheng V., Gutstein A., Wolak A., et. al.: Moving beyond binary grading of coronary arterial stenoses on coronary computed tomographic angiography: insights for the imager and referring clinician. JACC Cardiovasc Imaging 2008; 1: pp. 460-471.
17. Nieman K., Oudkerk M., Rensing B.J., et. al.: Coronary angiography with multi-slice computed tomography. Lancet 2001; 357: pp. 599-603.
18. Becker C.R., Ohnesorge B.M., Schoepf U.J., et. al.: Current development of cardiac imaging with multidetector-row CT. Eur J Radiol 2000; 36: pp. 97-103.
19. Madaj P., Gopal A., Hamirani Y., et. al.: The degree of stenosis on cardiac catheterization compared to calcified coronary segments on multi-detector row cardiac computed tomography MDCT. Acad Radiol 2010; 17: pp. 1001-1005.
20. Mendoza-Rodríguez V., Llerena L.R., Rodríguez-de la Vega A., et. al.: [Volume of coronary calcified plaques by computed tomography and presence of significant stenosis by coronary angiography]. Arch Cardiol Mex 2010; 80: pp. 181-186.
21. Ho J.S., Fitzgerald S.J., Stolfus L.L., et. al.: Relation of a coronary artery calcium score higher than 400 to coronary stenoses detected using multidetector computed tomography and to traditional cardiovascular risk factors. Am J Cardiol 2008; 101: pp. 1444-1447.
22. Kitamura A., Kobayashi T., Ueda K., et. al.: Evaluation of coronary artery calcification by multi-detector row computed tomography for the detection of coronary artery stenosis in Japanese patients. J Epidemiol 2005; 15: pp. 187-193.
23. Meyer M., Henzler T., Fink C., et. al.: Impact of coronary calcium score on the prevalence of coronary artery stenosis on dual source CT coronary angiography in caucasian patients with an intermediate risk. Acad Radiol 2012; 19: pp. 1316-1323.
24. Boll D.T., Merkle E.M., Paulson E.K., et. al.: Calcified vascular plaque specimens: assessment with cardiac dual-energy multidetector CT in anthropomorphically moving heart phantom. Radiology 2008; 249: pp. 119-126.
25. Sarwar A., Rieber J., Mooyaart E.A., et. al.: Calcified plaque: measurement of area at thin-section flat-panel CT and 64-section multidetector CT and comparison with histopathologic findings. Radiology 2008; 249: pp. 301-306.
26. Meijs M.F., de Vries J.J., Rutten A., et. al.: Does slice thickness affect diagnostic performance of 64-slice CT coronary angiography in stable and unstable angina patients with a positive calcium score?. Acta Radiol 2010; 51: pp. 427-430.
27. Leber A.W., Knez A., von Ziegler F., et. al.: Quantification of obstructive and nonobstructive coronary lesions by 64-slice computed tomography: a comparative study with quantitative coronary angiography and intravascular ultrasound. J Am Coll Cardiol 2005; 46: pp. 147-154.
28. Moselewski F., Ropers D., Pohle K., et. al.: Comparison of measurement of cross-sectional coronary atherosclerotic plaque and vessel areas by 16-slice multidetector computed tomography versus intravascular ultrasound. Am J Cardiol 2004; 94: pp. 1294-1297.
29. Marwan M., Pflederer T., Schepis T., et. al.: Coronary vessel and luminal area measurement using dual-source computed tomography in comparison with intravascular ultrasound: effect of window settings on measurement accuracy. J Comput Assist Tomogr 2011; 35: pp. 113-118.
30. Heuschmid M., Kuettner A., Schroeder S., et. al.: ECG-gated 16-MDCT of the coronary arteries: assessment of image quality and accuracy in detecting stenoses. AJR Am J Roentgenol 2005; 184: pp. 1413-1419.
31. Raff G.L., Chinnaiyan K.M., Share D.A., et. al.: Radiation dose from cardiac computed tomography before and after implementation of radiation dose-reduction techniques. JAMA 2009; 301: pp. 2340-2348.