
Rationale and Objectives
The aim of this study was to assess potential quality assurance (QA) issues in the diagnosis and characterization of adnexal masses on pelvic computed tomographic (CT) and magnetic resonance (MR) imaging studies.
Materials and Methods
Images from 128 women who had oophorectomies during a 16-month period with CT and/or MR studies within 5 years of surgery (145 CT scans from 103 women and 49 MR studies from 42 women, with 17 having both MR and CT studies) were reviewed by three radiologists who assigned QA scores of 0 (no QA issue), 1 (minor issue with minimal impact on clinical care), or 2 (major issue with potential impact on clinical care). The difficulty of diagnosis was assigned a score of 0 (very difficult diagnosis to make), 1 (difficult but possible to make the diagnosis), or 2 (diagnosis should be made). The incidence of adnexal QA issues was calculated using total CT and MR pelvic examinations performed on women during the interval.
Results
Twenty-nine QA issues were identified in 28 women in 17 of 145 CT studies (11.7%) and 12 of 49 MR examinations (24.5%) in women having adnexal surgery (17 of 11,194 [0.15%] of female pelvic CT studies and 12 of 603 [2.0%] of female pelvic MR studies performed in the time interval). Issues included missed lesions, lesions misidentified as leiomyomas, fat described in the lesion but not seen histologically, postmenopausal status of patient not considered, ultrasound correlation not recommended, and confusion of right and left sides.
Conclusion
Errors in CT and MR studies regarding the diagnosis and characterization of adnexal masses in a highly enriched population of women undergoing adnexal surgery are common. Knowledge of the types of QA issues found in CT and MR studies of adnexal masses should aid in decreasing future errors.
Ultrasound is the primary method for imaging adnexal masses, with magnetic resonance (MR) imaging often used as the secondary modality for further characterization of lesions seen on ultrasound. However, pelvic computed tomographic (CT) and MR studies performed for indications other than adnexal imaging often reveal adnexal pathology. Because adnexal lesions are not necessarily in the region of patients’ symptoms, these lesions can be overlooked. In addition, the CT and MR appearance of specific types of adnexal lesions might not be well recognized by general radiologists, and therefore, appropriate follow-up of lesions might not be recommended.
Peer review is increasingly used by radiologists to obtain feedback and reduce errors in the interpretation of imaging studies. However, little analysis of data from peer review has been published, including peer review for pelvic imaging.
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Computed Tomographic and MR QA Issues
Patient Modality Indication Age Finding as Described in Written Report QA Issue QA Details Median QA Score Difficulty Scores Final Diagnosis Interval Between Imaging and Surgery ∗ 1 CT Von Hippel-Lindau syndrome, renal and pancreatic hemangioma 55 3.8-cm left adnexal cyst, “could be further assessed with pelvic US” Inadequate follow-up recommendation This was not a simple cyst on CT: US recommendation should be stronger in a postmenopausal woman with 3.8-cm complex cyst 1 2, 2 Dermoid 17 mo 2 CT Flank/back pain, microscopic hematuria 58 3.3-cm adnexal mass (left in findings, right in impression) Inadequate description of location Reversed right and left in impression 1 2, NA Bilateral hydrosalpinx and paratubal cysts 1 mo 3 CT Left lower quadrant pain 49 12-cm simple-appearing adnexal cyst; recommended US or MR Inadequate follow-up recommendation MR should not be recommended when US is first-line study to assess internal characteristics of cyst 1 1, 2 Torsion 1 mo 4 CT Right lower quadrant pain 74 4.4-cm ovarian mass with mural calcification; “abnormal appearance of ovary” No differential diagnosis given 1 2, 2 Simple cyst, calcified arterioles 3 wk 5 CT Right lower quadrant pain radiating to back 59 1.7-cm low-attenuation focus in ovary Fat thought to be present on imaging, but no fat at pathology † 1 2, 2 Bilateral inclusion cysts and adhesions 1 mo 6 CT Left lower quadrant pain and fever 45 16-cm complex cystic structure, likely related to known left hydrosalpinx Inadequate description of location Only mentioned left side in bilateral process 1 2, 1 Bilateral tubo-ovarian abscess with intraovarian cysts and acute and chronic salpingitis 3 wk 7a (first exam) CT Left flank pain, hydronephrosis 39 9-cm uterine fibroid, eccentric to right Lack of correlation to prior studies New mass since 5 years previously 2 2, 2 Non-Hodgkin lymphoma 5 mo 7b (second exam) CT Left costovertebral angle pain 39 8.1-cm right pelvic mass, unchanged, likely fibroid Lack of correlation to older studies Compared to study 3 mo previously (7a) but not older studies 2 2, 1 Non-Hodgkin lymphoma 2 mo 8 CT Right lower quadrant pain, fever, abdominal distension 42 Tubular fluid–filled pelvic mass, likely hydrosalpinx, and pelvic free fluid Lack of clinical correlation No mention of infection in patient with fever, elevated white blood cell count 1 2, 2 Bilateral pyosalpinx, (right 10 cm, left 15 cm) 2 d 9a (first exam) CT Gluteal pain 51 Gluteal abscess vs sarcoma with adjacent fat stranding Missed lesion 2 2, 1 Dermoid (4 cm) 17 mo 9b (second exam) MR Left gluteal pain and soft-tissue mass 51 Gluteal abscess Missed lesion 2 2, 2 Dermoid (4 cm) 15 mo 10 CT Left lower quadrant pain 55 4.5-cm hemorrhagic cyst (right), 3.8-cm simple cyst (left); follow-up as clinically indicated Inadequate follow-up recommendation US indicated based on patient age and size of lesion 2 1, 2 Inclusion cyst (right), endometrioma (left) 17 mo 11 CT Lower abdominal pain 74 3.6-cm round dense mass in uterine fundus described as fibroid Miscategorization 2 0, 1 Serous papillary carcinoma 6 mo 12 CT Abdominal pain, fever 48 8.7-cm and 4.7-cm bilateral degenerating exophytic fibroids Miscategorization and lack of mention of nonvisualization of normal ovaries Lack of visualization of normal ovaries not mentioned in report 2 2, 2 Bilateral serous papillary carcinoma 12 d 13 CT Known gastrointestinal stromal tumor, evaluate for chemotherapy response 77 None Missed lesion 2 2, 2 Metastatic gastrointestinal stromal tumor (5 cm) 14 mo 14 CT Carcinoid tumor 35 “Prominent adnexa” unchanged since 2.5 mo previously Inadequate follow-up recommendation US was needed to characterize enlarged ovaries 2 2, 1 Metastatic carcinoid tumor (9 cm) 4 mo 15 CT Breast cancer and liver metastases 33 4.4-cm-thick walled cyst with asymmetric enhancement, suspicious for neoplasm Inadequate differential diagnosis Impression did not mention this cyst in patient with breast cancer 2 2, 2 Serous cystadenoma and paratubal cyst 2 mo 16 CT History of lymphoma 63 None Missed lesion 2 2, 2 Serous cystadenoma (3.2 cm) 11 mo 17 MR Ovarian cyst seen on US at 20-wk gestational age 34 8.5-cm adnexal cyst, loss of signal on out-of-phase T1 and fat-saturated T1 Fat seen on MR but not at pathology † 1 2, 0 Epidermal cyst, no fat present 4 mo 18 MR Elevated liver function test results 51 None Missed lesion, lack of comparison to prior studies Known adnexal cyst not mentioned 1 2, 2 Serous cystadenoma (4.4 cm) 7 mo 19 MR Echogenic renal mass and ovarian cyst 57 1.5-cm right cyst, 2.0-cm left cyst, no nodularity or enhancement Missed lesion Solid Brenner tumor not mentioned 1 1, 1 Serous cystadenoma (right), Brenner tumor (left 2 cm) 3 mo 20 MR Back pain, known sacral/retroperitoneal mass 57 4.6-cm necrotic retroperitoneal mass, 1.3-cm endometrial lesion Missed lesion Necrotic ovarian mass with 7-mm solid nodule 1 2, 0 Metastatic endometrial cancer 2 mo 21 MR Adnexal cyst seen on US at 7-wk gestational age 34 7.1-cm heterogeneous adnexal mass with small area of fat signal intensity Fat mentioned on MR but not seen at pathology † Review of pathology showed a classic mucinous cystadenoma: the dumbbell-shaped lesion had fat outside the cystic components, misinterpreted as being within the cyst 2 2, 2 Mucinous cystadenoma 7 mo 22 MR Cervical cancer staging 49 8-cm adnexal cyst with smooth wall with mild enhancement and thin septation, corpus luteum, or cystadenoma Inadequate differential diagnosis 1 2, 2 Hydrosalpinx, salpingitis 1 mo 23 MR Adnexal mass seen on US 64 3.1-cm heterogeneous mass, enhancement similar to myometrium, suggests fibroid Miscategorization No fibroid seen at surgery 2 2, 1 Paratubal cyst 12 d 24 MR Adnexal mass, fibroids 49 Enlarged cystic ovaries Inadequate differential diagnosis No mention of possible neoplasm 2 2, 2 Bilateral dermoids (right 7 cm, left 6 cm) 1 mo 25 MR Enlarged uterus on hysterosalpingogram 35 3.3-cm intramural/submucosal uterine lesion Miscategorization Adenomyosis called fibroid 1 1, 1 Adenomyosis 5 mo 26 MR Pelvic/rectal pain 59 Bilateral ovarian cysts, no pelvic abnormalities Inadequate follow-up recommendation Cysts in a postmenopausal woman should be further characterized by US; report gave no description of size of cysts 2 2, 2 Peritoneal inclusion cyst (right 5 cm, left 8 cm) 57 mo 27 MR Fibroids 49 3.9-cm right lesion with low-signal layering; normal left ovary Inadequate description of location; inadequate comparison to prior studies US had shown endometrioma on left 2 2, 1 Endometrioma (left 4 cm) 3 mo
CT, computed tomography; MR, magnetic resonance; NA, not applicable (the reviewer felt that the scoring system did not cover this issue); QA, quality assurance; US, ultrasound.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
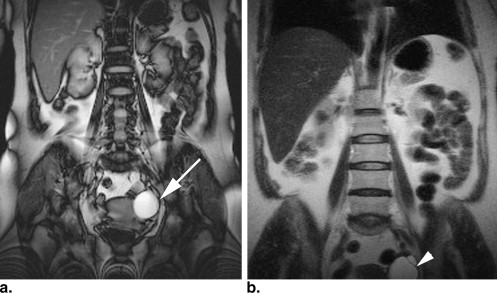


![Figure 7, A 34-year-old woman at 20-week gestational age with an adnexal cyst seen on obstetric ultrasound. (a) Axial T2-weighted single-shot fast spin-echo (repetition time [TR], 727 ms; echo time [TE], 60 ms; matrix size, 256 × 160; slice thickness, 4 mm) magnetic resonance image shows an 8.5-cm right adnexal cyst with a small mural nodule (arrow) anteriorly. Axial gradient-echo (GRE) T1-weighted in-phase image (b) (TR, 205 ms; TE, 4.4 ms; matrix size, 256 × 160; slice thickness, 5 mm) shows high signal intensity in the nodule (arrow) compared to the low–signal intensity fluid in the cyst. Because of the loss of signal intensity within the nodule (arrow) on the T1-weighted opposed phase (TR, 205 ms; TE, 2.2 ms; matrix size, 256 × 160; slice thickness, 5 mm) (c) and fat-saturated GRE (TR, 180 ms; TE, 4.2 ms; matrix size, 256 × 160; slice thickness, 5 mm) (d) images, this cyst was called a dermoid. However, no fat was identified histologically, and the final diagnosis was epidermoid cyst.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/PatternsofMisinterpretationofAdnexalMassesonCTandMRinanAcademicRadiologyDepartment/6_1s20S1076633209001470.jpg)

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Asch E., Levine D.: The spectrum of appearance of endometriosis. J Ultrasound Med 2007; 26: pp. 993-1002.
2. Asch E., Levine D., Hecht J.: Histologic, operative, and imaging correlations of adnexalmasses. J Ultrasound Med 2008; 3: pp. 327-342.
3. Asch E., Levine D., Mehta T.S., Kim Y., Hecht J.: Assessing factors that impact the quality of performance and interpretation of sonography of adnexal masses. J Ultrasound Med 2008; 27: pp. 721-728.
4. Tsili A.C., Tsampoulas C., Charisiadi A.: Adnexal masses: accuracy of detection and differentiation with multidetector computed tomography. Gynecol Oncol 2008; 110: pp. 22-31.
5. Scoutt L.M., McCarthy S.M., Lange R., et. al.: MR evaluation of clinically suspected adnexal masses. J Comput Assist Tomogr 1994; 18: pp. 609-618.
6. Sohaib S.A., Sahdev A., Van Trappen P., et. al.: Characterization of adnexal mass lesions on MR imaging. AJR Am J Roentgenol 2003; 180: pp. 1297-1304.
7. Kalish G.M., Patel M.D., Gunn M.L., et. al.: Computed tomographic and magnetic resonance features of gynecologic abnormalities in women presenting with acute or chronic abdominal pain. Ultrasound Q 2007; 23: pp. 167-175.
8. Slanetz P.J., Hahn P.F., Hall D.A., et. al.: The frequency and significance of adnexal lesions incidentally revealed by CT. AJR Am J Roentgenol 1997; 168: pp. 647-650.
9. Togashi K.: Ovarian cancer: the clinical role of US, CT, and MRI. Eur Radiol 2003; 13: pp. L87-L104.
10. Friedman A.C., Pyatt R.S., Hartman D.S., et. al.: CT of benign cystic teratomas. AJR Am J Roentgenol 1982; 138: pp. 659-665.
11. Laing F.C., Van Dalsem F.V., Marks W.M., et. al.: Dermoid cysts of the ovary: their ultrasonographic appearances. Obstet Gynecol 1981; 57: pp. 99-104.
12. Sandler M.A., Silver T.M., Karo J.J.: Gray-scale ultrasonic features of ovarian teratomas. Radiology 1979; 131: pp. 705-709.
13. Casillas J., Joseph R.C., Guerra J.J.: CT appearance of uterine leiomyomas. Radiographics 1990; 10: pp. 999-1007.
14. Sanders R.C., McNeil B.J., Finberg H.J., et. al.: A prospective study of computed tomography and ultrasound in the detection and staging of pelvic masses. Radiology 1983; 146: pp. 439-442.
15. Walsh J.W., Rosenfeld A.T., Jaffe C.C., et. al.: Prospective comparison of ultrasound and computed tomography in the evaluation of gynecologic pelvic masses. AJR Am J Roentgenol 1978; 131: pp. 955-960.
16. Mawhinney R.R., Powell M.C., Worthington B.S., et. al.: Magnetic resonance imaging of benign ovarian masses. Br J Radiol 1988; 61: pp. 179-186.
17. Togashi K., Nishimura K., Itoh K., et. al.: Ovarian cystic teratomas: MR imaging. Radiology 1987; 162: pp. 669-673.
18. Yamashita Y., Hatanaka Y., Torashima M., et. al.: Mature cystic teratomas of the ovary without fat in the cystic cavity: MR features in 12 cases. AJR Am J Roentgenol 1994; 163: pp. 613-616.
19. Smith R.C., Lange R.C., McCarthy S.M.: Chemical shift artifact: dependence on shape and orientation of the lipid-water interface. Radiology 1991; 181: pp. 225-229.
20. Chatzistamou I., Kairi-Vasillatou E., Hasiakos D., et. al.: Retrospective study of teratomas of the ovary reveals a high incidence of epidermoid cysts. Gynecol Oncol 2006; 101: pp. 548-549.
21. Shinya T., Joja I., Hashimura S., et. al.: Magnetic resonance imaging features of epidermoid cyst of the ovaries: magnetic resonance and computed tomography findings. J Comput Assist Tomogr 2006; 30: pp. 906-909.
22. Takeshita M., Kubo O., Hiyama H., et. al.: Magnetic resonance imaging and quantitative analysis of contents of epidermoid and dermoid cysts. Neurol Med Chir (Tokyo) 1994; 34: pp. 436-439.
23. Allbery S.M., Chaljub G., Cho N.L., Rassekh C.H., John S.D., Guinto F.C.: MR imaging of nasal masses. Radiographics 1995; 15: pp. 1311-1327.
24. McKinlay S.M., Brambilla D.J., Posner J.G.: The normal menopause transition. Maturitas 1992; 14: pp. 103-115.
25. McKinlay S.M., Bifano N.L., McKinlay J.B.: Smoking and age at menopause in women. Ann Intern Med 1985; 103: pp. 350-356.
26. Levine D.: What is the significance of the incidental discovery of a unilocular ovarian cyst in a postmenopausal woman (either with or without a family history of ovarian cancer) during a pelvic sonographic examination to exclude ovarian carcinoma?. AJR Am J Roentgenol 1994; 163: pp. 215-216.
27. Patel M.D., Dubinsky T.J.: Reimaging the female pelvis with ultrasound after CT: general principles. Ultrasound Q 2007; 23: pp. 177-187.
28. Orel S.G., Kay N., Reynolds C., Sullivan D.C.: BI-RADS categorization as a predictor of malignancy. Radiology 1999; 211: pp. 845-850.