
Rationale and Objectives
To compare prostate morphology, image quality, and diagnostic performance of 1.5-T endorectal coil magnetic resonance (MR) imaging (MRI) and 3.0-T nonendorectal coil MRI in patients with prostate cancer.
Materials and Methods
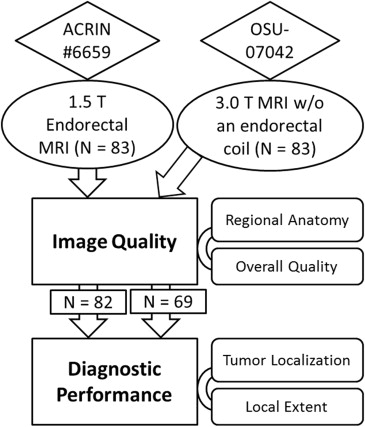
MR images obtained of 83 patients with prostate cancer using 1.5-T MRI systems with an endorectal coil were compared to images collected from 83 patients with a 3.0-T MRI system. Prostate diameters were measured, and image quality was evaluated by one American Board of Radiology (ABR)–certified radiologist (reader 1) and one ABR-certified diagnostic medical physicist (reader 2). The likelihood of the presence of peripheral zone cancer in each sextant and local extent was rated and compared to histopathologic findings.
Results
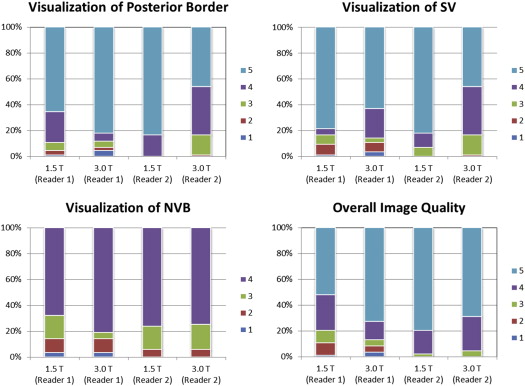
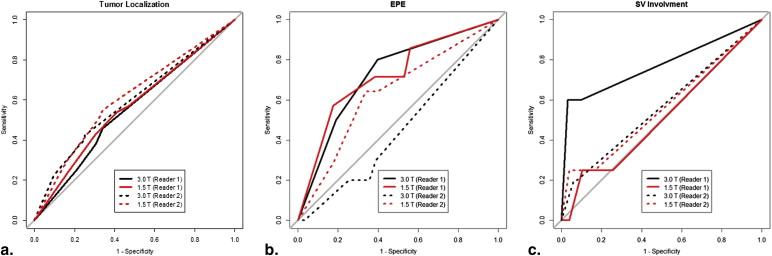
Prostate anterior–posterior diameter measured by both readers was significantly shorter with 1.5-T endorectal MRI than with 3.0-T MRI. The overall image quality score difference was significant only for reader 1. Both readers found that the two MRI systems provided a similar diagnostic accuracy in cancer localization, extraprostatic extension, and seminal vesicle involvement.
Conclusions
Nonendorectal coil 3.0-T MRI provides prostate images that are natural in shape and that have comparable image quality to those obtained at 1.5 T with an endorectal coil, but not superior diagnostic performance. These findings suggest an opportunity exists for improving technical aspects of the 3.0-T prostate MRI.
Prostate cancer is the second most common cause of cancer death among American men. The American Cancer Society estimated that 233,000 new cases of prostate cancer would be diagnosed in 2014, and approximately 29,480 men would die of the disease . Magnetic resonance (MR) imaging (MRI), with excellent soft-tissue contrast, provides high resolution images of the pelvis for use in prostate cancer management .
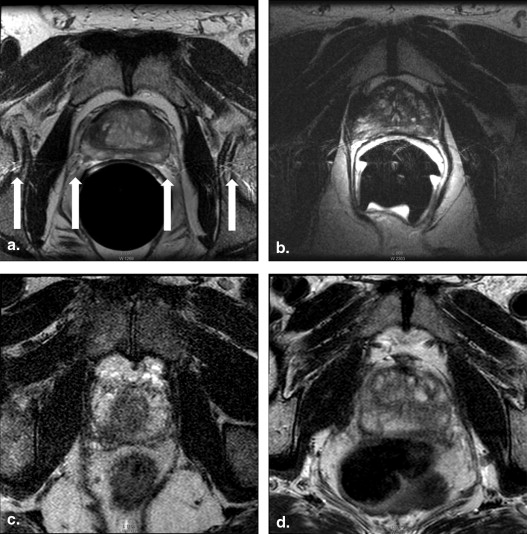
The use of an endorectal coil is an essential part of the prostate 1.5-T MRI protocol in the clinical diagnosis of prostate cancer . An endorectal coil is inserted tightly against the prostate during the MRI examination to increase image resolution and improve staging accuracy . However, the endorectal coil leads to deformity in the prostate contour, and the anatomic distortion resulting from it can potentially hinder the diagnosis and pathology correlation . The changes in prostate shape and volume after the introduction of an endorectal coil may cause difficulties in MRI–computed tomography fusion and radiotherapy planning . Another limitation is that patients with rectal stenosis or immediately after surgery or radiotherapy may not be good candidates for the use of the endorectal coil during MR examination .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Study Design and Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MR Imaging Protocol
Get Radiology Tree app to read full this article<
Table 1
Parameters for T2-weighted MR Imaging
Parameters Axial T2-weighted Fast Spin Echo Coronal T2-weighted Fast Spin Echo 1.5-T Endorectal 3.0 T 1.5-T Endorectal 3.0 T Coil Torso phased-array, endorectal 32-channel phased-array Torso phased-array, endorectal 32-channel phased-array TR (ms)/TE (ms) 4000–6600/90–150 3488–4400/100 4000–6500/90–150 2138–2685/100 Section thickness 3 3 3 3 Intersection gap (mm) 0–1 0.3 0–1 0.5 Field of view (mm) 100–142 140 100–140 260 Frequency direction Anteroposterior Anteroposterior Anteroposterior or superoinferior Superoinferior Matrix 256 × 192 192 × 154 256 × 192 304 × 294 Number of signals acquired 1.5–2 2 1.5–3 2 Echo train length 8–16 14 8–16 14
MR, magnetic resonance; TE, echo time; TR, repetition time.
Get Radiology Tree app to read full this article<
Image and Histopathology Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Qualitative Evaluation of Image Quality
Visualization of Posterior Border Visualization of Seminal Vesicles 5. Well delineated 5. Margins and septations seen 4. 75%–100% of margin clearly seen 4. Margins seen, septations poorly defined 3. 50%–75% of margin clearly seen 3. Septations seen, margins poorly defined 2. 25%–50% of margin clearly seen 2. Poorly defined 1. <25% of margin clearly seen 1. Unreadable Visualization of Neurovascular Bundle Overall Image Quality Rating 4. Seen well on both sides 5. Excellent 3. Seen well on one side 4. Very good 2. Seen suboptimally on both sides 3. Good 1. Unreadable 2. Fair 1. Poor
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
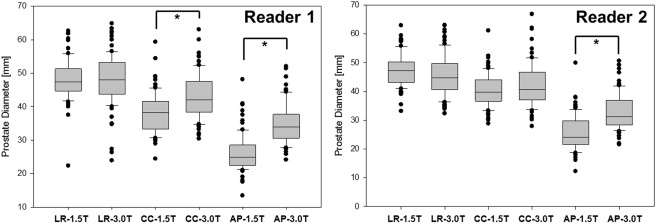
Table 3
Comparison of Prostate Diameter Measurement
Reader 1: Radiologist Reader 2: Physicist 1.5-T Endorectal 3.0 T_P_ Value ∗ 1.5-T Endorectal 3.0 T_P_ Value ∗ Prostate diameter measurement Left–right (mm) 48.0 ± 6.0 48.1 ± 7.6 .553 (NS) 47.5 ± 5.6 45.7 ± 7.1 .039 Cranial–caudal (mm) 38.3 ± 6.0 43.2 ± 6.9 <.001 40.3 ± 5.7 42.1 ± 7.6 .179 (NS) Anterior–posterior (mm) 26.2 ± 5.5 35.0 ± 5.9 <.001 25.5 ± 6.0 32.8 ± 6.3 <.001 LR/CC ratio 1.27 ± 0.18 1.13 ± 0.19 <.001 1.19 ± 0.17 1.10 ± 0.18 <.001 LR/AP ratio 1.88 ± 0.30 1.40 ± 0.23 <.001 1.93 ± 0.36 1.41 ± 0.19 <.001 Image quality scoring result Posterior border 4.48 ± 0.86 4.58 ± 1.04 .041 4.83 ± 0.38 4.81 ± 0.45 .946 (NS) SV 4.51 ± 1.03 4.34 ± 1.09 .069 (NS) 4.75 ± 0.58 4.28 ± 0.77 <.001 NVB † 3.49 ± 0.83 3.63 ± 0.82 .101 (NS) 3.70 ± 0.58 3.69 ± 0.58 .869 (NS) Overall image quality 4.19 ± 1.04 4.47 ± 1.04 .014 4.77 ± 0.48 4.64 ± 0.58 .107 (NS) AUCs for diagnostic performance Sextant tumor localization 0.5664 0.5521 .701 (NS) 0.6095 0.5932 .628 (NS) Extracapsular extension 0.7206 0.7250 .968 (NS) 0.6334 0.4475 .088 (NS) SV involvement 0.5112 0.7714 .133 (NS) 0.5577 0.5625 .975 (NS)
AP, anterior–posterior; AUCs, area under the receiver operating characteristic curves; CC, cranial–caudal; LR, left–right; NS, not significant; NVB, neurovascular bundle; SV, seminal vesicles.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Siegel R., Ma J., Zou Z., et. al.: Cancer statistics, 2014. CA Cancer J Clin 2014; 64: pp. 9-29.
2. Mazaheri Y., Shukla-Dave A., Muellner A., et. al.: MRI of the prostate: clinical relevance and emerging applications. J Magn Reson Imaging 2011; 33: pp. 258-274.
3. Hricak H., Choyke P.L., Eberhardt S.C., et. al.: Imaging prostate cancer: a multidisciplinary perspective. Radiology 2007; 243: pp. 28-53.
4. Hricak H., White S., Vigneron D., et. al.: Carcinoma of the prostate gland: MR imaging with pelvic phased-array coils versus integrated endorectal–pelvic phased-array coils. Radiology 1994; 193: pp. 703-709.
5. Rajesh A., Coakley F.V.: MR imaging and MR spectroscopic imaging of prostate cancer. Magn Reson Imaging Clin N Am 2004; 12: pp. 557-579.
6. Heijmink S.W., Scheenen T.W., van Lin E.N., et. al.: Changes in prostate shape and volume and their implications for radiotherapy after introduction of endorectal balloon as determined by MRI at 3T. Int J Radiat Oncol Biol Phys 2009; 73: pp. 1446-1453.
7. Hensel J.M., Menard C., Chung P.W., et. al.: Development of multiorgan finite element-based prostate deformation model enabling registration of endorectal coil magnetic resonance imaging for radiotherapy planning. Int J Radiat Oncol Biol Phys 2007; 68: pp. 1522-1528.
8. Park B.K., Kim B., Kim C.K., et. al.: Comparison of phased-array 3.0-T and endorectal 1.5-T magnetic resonance imaging in the evaluation of local staging accuracy for prostate cancer. J Comput Assist Tomogr 2007; 31: pp. 534-538.
9. Rouviere O., Hartman R.P., Lyonnet D.: Prostate MR imaging at high-field strength: evolution or revolution?. Eur Radiol 2006; 16: pp. 276-284.
10. Beyersdorff D., Taymoorian K., Knosel T., et. al.: MRI of prostate cancer at 1.5 and 3.0 T: comparison of image quality in tumor detection and staging. Am J Roentgenol 2005; 185: pp. 1214-1220.
11. Sosna J., Pedrosa I., Dewolf W.C., et. al.: MR imaging of the prostate at 3 Tesla: comparison of an external phased-array coil to imaging with an endorectal coil at 1.5 Tesla. Acad Radiol 2004; 11: pp. 857-862.
12. Torricelli P., Cinquantini F., Ligabue G., et. al.: Comparative evaluation between external phased array coil at 3 T and endorectal coil at 1.5 T: preliminary results. J Comput Assist Tomogr 2006; 30: pp. 355-361.
13. Tahmasebi A.M., Sharifi R., Agarwal H.K., et. al.: A statistical model-based technique for accounting for prostate gland deformation in endorectal coil-based MR imaging. Conf Proc IEEE Eng Med Biol Soc 2012; 2012: pp. 5412-5415.
14. Weinreb J.C., Blume J.D., Coakley F.V., et. al.: Prostate cancer: sextant localization at MR imaging and MR spectroscopic imaging before prostatectomy–results of ACRIN prospective multi-institutional clinicopathologic study. Radiology 2009; 251: pp. 122-133.
15. Jia G., Abaza R., Williams J.D., et. al.: Amide proton transfer MR imaging of prostate cancer: a preliminary study. J Magn Reson Imaging 2011; 33: pp. 647-654.
16. Pantanowitz L., Sinard J.H., Henricks W.H., et. al.: Validating whole slide imaging for diagnostic purposes in pathology: guideline from the College of American Pathologists Pathology and Laboratory Quality Center. Arch Pathol Lab Med 2013; 137: pp. 1710-1722.
17. Robin X., Turck N., Hainard A., et. al.: pROC: an open-source package for R and S+ to analyze and compare ROC curves. Bmc Bioinformatics 2011; 12: pp. 77.
18. Wu X., Dibiase S.J., Gullapalli R., et. al.: Deformable image registration for the use of magnetic resonance spectroscopy in prostate treatment planning. Int J Radiat Oncol Biol Phys 2004; 58: pp. 1577-1583.
19. Bharatha A., Hirose M., Hata N., et. al.: Evaluation of three-dimensional finite element-based deformable registration of pre- and intraoperative prostate imaging. Med Phys 2001; 28: pp. 2551-2560.
20. Pursley J., Risholm P., Fedorov A., et. al.: A Bayesian nonrigid registration method to enhance intraoperative target definition in image-guided prostate procedures through uncertainty characterization. Med Phys 2012; 39: pp. 6858-6867.
21. Hirose M., Bharatha A., Hata N., et. al.: Quantitative MR imaging assessment of prostate gland deformation before and during MR imaging-guided brachytherapy. Acad Radiol 2002; 9: pp. 906-912.
22. Schreibmann E., Xing L.: Narrow band deformable registration of prostate magnetic resonance imaging, magnetic resonance spectroscopic imaging, and computed tomography studies. Int J Radiat Oncol Biol Phys 2005; 62: pp. 595-605.
23. Brock K.K., Nichol A.M., Menard C., et. al.: Accuracy and sensitivity of finite element model-based deformable registration of the prostate. Med Phys 2008; 35: pp. 4019-4025.
24. Husband J.E., Padhani A.R., MacVicar A.D., et. al.: Magnetic resonance imaging of prostate cancer: comparison of image quality using endorectal and pelvic phased array coils. Clin Radiol 1998; 53: pp. 673-681.
25. Heijmink S.W., Futterer J.J., Hambrock T., et. al.: Prostate cancer: body-array versus endorectal coil MR imaging at 3 T–comparison of image quality, localization, and staging performance. Radiology 2007; 244: pp. 184-195.
26. Rosenkrantz A.B., Bennett G.L., Doshi A., et. al.: T2-weighted imaging of the prostate: impact of the BLADE technique on image quality and tumor assessment. Abdom Imaging 2014;
27. Turkbey B., Merino M.J., Gallardo E.C., et. al.: Comparison of endorectal coil and nonendorectal coil T2W and diffusion-weighted MRI at 3 Tesla for localizing prostate cancer: correlation with whole-mount histopathology. J Magn Reson Imaging 2013;
28. Bloch B.N., Rofsky N.M., Baroni R.H., et. al.: 3 Tesla magnetic resonance imaging of the prostate with combined pelvic phased-array and endorectal coils: initial experience. Acad Radiol 2004; 11: pp. 863-867.
29. Futterer J.J., Scheenen T.W., Huisman H.J., et. al.: Initial experience of 3 tesla endorectal coil magnetic resonance imaging and 1H-spectroscopic imaging of the prostate. Invest Radiol 2004; 39: pp. 671-680.
30. Kim D.Y., Schnall M.D., Rosen M.A., et. al.: Prostate MR imaging at 3T with a longitudinal array endorectal surface coil and phased array body coil. J Magn Reson Imaging 2008; 27: pp. 1327-1330.
31. Futterer J.J., Heijmink S.W., Scheenen T.W., et. al.: Prostate cancer localization with dynamic contrast-enhanced MR imaging and proton MR spectroscopic imaging. Radiology 2006; 241: pp. 449-458.
32. Futterer J.J., Engelbrecht M.R., Jager G.J., et. al.: Prostate cancer: comparison of local staging accuracy of pelvic phased-array coil alone versus integrated endorectal-pelvic phased-array coils. Local staging accuracy of prostate cancer using endorectal coil MR imaging. EurRadiol 2007; 17: pp. 1055-1065.
33. Serai S.D., Merrow A.C., Kline-Fath B.M.: Fetal MRI on a multi-element digital coil platform. Pediatr Radiol 2013; 43: pp. 1213-1217.
34. Dickinson L., Ahmed H.U., Allen C., et. al.: Magnetic resonance imaging for the detection, localisation, and characterisation of prostate cancer: recommendations from a European consensus meeting. Eur Urol 2011; 59: pp. 477-494.