
Rationale and Objectives
Preoperative colonic evaluation is often inadequate because of cancer stenosis making a full conventional colonoscopy (CC) impossible. In several studies, cancer stenosis has been shown in up to 16%–34% of patients with colorectal cancer. The purpose of this study was to prospectively evaluate the completion rate of preoperative colonic evaluation and the quality of perioperative colonic evaluation using magnetic resonance colonography (MRC) in patients with rectal cancer.
Materials and Methods
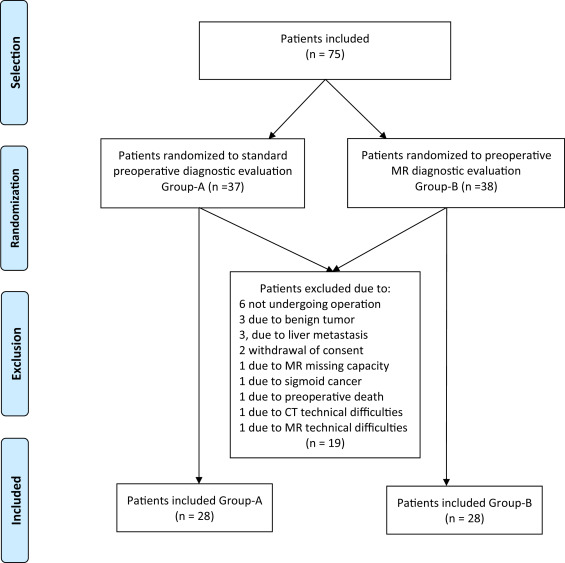
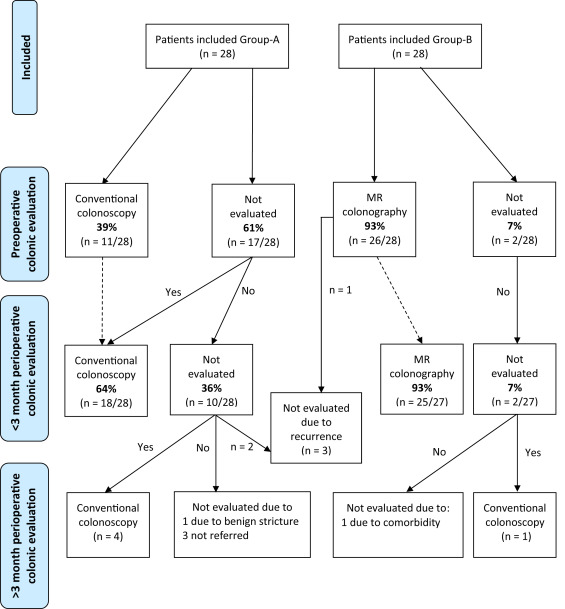
Patients diagnosed with rectal cancer were randomized to either group A: standard preoperative diagnostic work-up or group B: preoperative MR diagnostic work-up (standard preoperative diagnostic work-up + MRC). A complete and adequate perioperative clean-colon evaluation (PCE) was defined as either a complete preoperative colonic evaluation or a complete colonic evaluation within 3 months postoperatively.
Results
Twenty-eight patients were randomized to group A and 28 to group B. Complete preoperative colonic evaluation with CC was achieved in 39% patients in group A and 93% for group B (Fisher’s exact test, P < .001). PCE with CC was achieved in 64% and 93% in groups A and B, respectively (Fisher’s exact test, P = .02). In group A, one synchronous cancer was found by CC. However, the location was misjudged as a sigmoid cancer. In group B, two synchronous cancers were found in the same patient who had an insufficient preoperative CC due to an obstructing rectal cancer.
Conclusions
MRC is a valuable tool and is recommended as part of the standard preoperative evaluation for patients with rectal cancer.
Introduction
Colorectal cancer is the third most common cancer in men and the second in women worldwide. At this time, it is estimated that 1.361 million new cases and 694 million deaths are caused every year by colorectal cancer, and most patients die from synchronous and metachronous lesions . Thus, a thorough preoperative (PREOP) diagnostic work-up is necessary. It is often comprised of a computed tomography (CT) of the thorax and abdomen along with colonic evaluation. In case of rectum cancer, an evaluation of the tumor by transrectal ultrasound or magnetic resonance (MR) is also performed. The PREOP diagnostic work-up is performed to find synchronous lesions; liver metastases are found in up to 19% of patients , colon cancer in 2%–11% and up to 61% of patients with polyps . The diagnosis of synchronous liver metastases is primarily used for determination of resectability, whereas the diagnosis of synchronous colonic lesions is for planning of surgical strategy. The presence of synchronous colonic lesions in patients with colon cancer was described already in 1922 ; more than 30 years ago, it was recommended to do PREOP colonic evaluation . For the time being, it recommended that the colonic evaluation is done by conventional colonoscopy (CC) because of the high sensitivity, direct visualization of the mucosa, and therapeutic ability for resecting polyps. However, inadequate colonic evaluation is often seen because of lack of resources, acute surgery, poor bowel preparation, adhesions, pain, and most importantly, cancer stenosis making a full CC impossible. In several studies, cancer stenosis has been shown in up to 16%–34% of patients with colorectal cancer .
The purpose of this study was to prospectively evaluate the completion rate of PREOP colonic evaluation. Furthermore, to evaluate the quality of perioperative clean-colonic evaluation (PCE) using either standard perioperative colonic evaluation versus magnetic resonance colonography (MRC) in patients with rectal cancer.
Materials and methods
Get Radiology Tree app to read full this article<
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Patient Bowel Preparation
Get Radiology Tree app to read full this article<
MR Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analyses
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conventional Colonoscopy
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Complete Colonic Evaluation
Get Radiology Tree app to read full this article<
Results
Patient Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Evaluation
Colon Evaluation
Get Radiology Tree app to read full this article<
Table 1
Modality Used for Preoperative Colonic Evaluation
Frequency Percent Group A Rectoscopy 1 3.6 Sigmoidoscopy 12 42.9 Colonoscopy 11 39.3 Rectocopy due to stricture 2 7.1 Sigmoidoscopy due to stricture 3 10.7 Total 28 100.0 Group B Rectoscopy 2 7.1 Sigmoidoscopy 10 35.7 Colonoscopy 10 35.7 Rectoscopy due to stricture 3 10.7 Sigmoidoscopy due to stricture 3 10.7 Total 28 100.0
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MR Colonography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Colonic Findings
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. International agency for research on cancer: GLOBOCAN 2012: Estimated cancer incidence, mortality and prevalence worldwide in 2012.2014. Ref Type: Online Source
2. Scheele J., Stangl R., Altendorf-Hofmann A.: Hepatic metastases from colorectal carcinoma: impact of surgical resection on the natural history. Br J Surg 1990; 77: pp. 1241-1246.
3. Heald R.J., Bussey H.J.: Clinical experiences at St. Mark’s Hospital with multiple synchronous cancers of the colon and rectum. Dis Colon Rectum 1975; 18: pp. 6-10.
4. Gordon-Watson C.: Specimen showing carcinoma of the pelvic colon and rectum co-existing and causing acute obstruction. Proc R Soc Med 1922; 15: pp. 92-93.
5. Maxfield R.G.: Colonoscopy as a routine preoperative procedure for carcinoma of the colon. Am J Surg 1984; 147: pp. 477-480.
6. Carraro P.G., Segala M., Cesana B.M., et. al.: Obstructing colonic cancer: failure and survival patterns over a ten-year follow-up after one-stage curative surgery. Dis Colon Rectum 2001; 44: pp. 243-250.
7. Phillips R.K., Hittinger R., Fry J.S., et. al.: Malignant large bowel obstruction. Br J Surg 1985; 72: pp. 296-302.
8. Isler J.T., Brown P.C., Lewis F.G., et. al.: The role of preoperative colonoscopy in colorectal cancer. Dis Colon Rectum 1987; 30: pp. 435-439.
9. Achiam M.P., Burgdorf S.K., Wilhelmsen M., et. al.: Inadequate preoperative colonic evaluation for synchronous colorectal cancer. Scand J Surg 2009; 98: pp. 62-67.
10. Adloff M., Arnaud J.P., Bergamaschi R., et. al.: Synchronous carcinoma of the colon and rectum: prognostic and therapeutic implications. Am J Surg 1989; 157: pp. 299-302.
11. Askew A., Ward M., Cowen A.: The influence of colonoscopy on the operative management of colorectal cancer. Med J Aust 1986; 145: pp. 254-255.
12. Fenlon H.M., McAneny D.B., Nunes D.P., et. al.: Occlusive colon carcinoma: virtual colonoscopy in the preoperative evaluation of the proximal colon. Radiology 1999; 210: pp. 423-428.
13. Howard M.L., Greene F.L.: The effect of preoperative endoscopy on recurrence and survival following surgery for colorectal carcinoma. Am Surg 1990; 56: pp. 124-127.
14. Dasmahapatra K.S., Lopyan K.: Rationale for aggressive colonoscopy in patients with colorectal neoplasia. Arch Surg 1989; 124: pp. 63-66.
15. Tate J.J., Rawlinson J., Royle G.T., et. al.: Pre-operative or postoperative colonic examination for synchronous lesions in colorectal cancer. Br J Surg 1988; 75: pp. 1016-1018.
16. Vignati P., Welch J.P., Cohen J.L.: Endoscopic localization of colon cancers. Surg Endosc 1994; 8: pp. 1085-1087.
17. Cho Y.B., Lee W.Y., Yun H.R., et. al.: Tumor localization for laparoscopic colorectal surgery. World J Surg 2007; 31: pp. 1491-1495.
18. Wexner S.D., Cohen S.M., Ulrich A., et. al.: Laparoscopic colorectal surgery–are we being honest with our patients?. Dis Colon Rectum 1995; 38: pp. 723-727.
19. Achiam M.P., Holst Andersen L.P., Klein M., et. al.: Preoperative evaluation of synchronous colorectal cancer using MR colonography. Acad Radiol 2009; 16: pp. 790-797.
20. Morrin M.M., Farrell R.J., Raptopoulos V., et. al.: Role of virtual computed tomographic colonography in patients with colorectal cancers and obstructing colorectal lesions. Dis Colon Rectum 2000; 43: pp. 303-311.
21. Zijta F.M., Bipat S., Stoker J.: Magnetic resonance (MR) colonography in the detection of colorectal lesions: a systematic review of prospective studies. Eur Radiol 2010; 20: pp. 1031-1046.
22. van der Paardt M.P., Zijta F.M., Boellaard T.N., et. al.: Magnetic resonance colonography with automated carbon dioxide insufflation: diagnostic accuracy and distension. Eur J Radiol 2014; 83: pp. 743-750.
23. Leslie A., Carey F.A., Pratt N.R., et. al.: The colorectal adenoma-carcinoma sequence. Br J Surg 2002; 89: pp. 845-860.