
Rationale and Objectives
Malignant mesothelioma (MM) of the pleura is an aggressive and often fatal neoplasm. Because MM frequently demonstrates marked angiogenesis, it may be responsive to antiangiogenic therapy, but effective methods for selecting and monitoring of patients are further needed. We employed dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) and quantitative immunohistochemistry (IHC) to characterize the microvascularity of MM using both a physiologic and ultrastructural method.
Materials and Methods
Nineteen patients diagnosed with MM were enrolled and DCE-MRI was performed before antiangiogenic treatment. For each patient, tumor regions were characterized by their DCE-MRI–derived pharmacokinetic parameters (Amp, k ep , k el ), which were also compared to those of normal tissue (aorta, liver, spleen, and muscle). In addition, quantitative IHC of representative samples was performed with CD-34 staining to compare the calculated microvessel density (MVD) results with DCE-MRI results.
Results
MM demonstrated markedly abnormal pharmacokinetic properties compared with normal tissues. Among the parameters tested, Amp was significantly different in MM ( P ≤ .001) compared to normal organs. Despite the observation that the MVD of mesotheliomas in this series was high compared to other tumors, DCE-MRI pharmacokinetic parameters had a moderately positive correlation with MVD ( r = 0.5).
Conclusions
DCE-MRI and IHC can be used in patients with MM to visualize tumor microvascularity and to characterize tumor heterogeneity. DCE-MRI and IHC results positively correlated, though moderately, but these two methods present as essential tumor biomarkers. This multimodal characterization may be useful in selecting possible tumor subtypes that would benefit from antiangiogenic therapy.
Malignant epithelioid mesothelioma (MM) is one of the three main types of mesotheliomas. It is an aggressive tumor of the pleura and often fatal. Most, if not all, MMs are associated with prior exposure to asbestos ( ). Although this epithelioid type has the best prognosis, standard treatment regimens, including surgery, chemotherapy, and radiation are often unsuccessful (median survival 9 months). Nevertheless, long-term survivors have been reported, and new chemotherapy and multimodal regimens show promising results ( ).
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) is a new biomarker imaging technique and a method of characterizing tumor’s neovascularity in situ ( ) as well as assessing the effects of therapy on tumor angiogenesis ( ). DCE-MRI is a noninvasive procedure in which sequential images with high spatial and temporal resolution are obtained to observe the kinetics of contrast media arrival and clearance through the tumor microcirculation and adjacent tissues. The contrast agent enhancement pattern enables visualization, characterization, and quantification of lesion microcirculation ( ). DCE-MRI parameters allowed the prediction of response to therapy in some cases ( ); however, not all tumors have shown strong correlations between their DCE-MRI patterns and their angiogenic expression.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Material and methods
Patients and Diagnostic Evaluation
Get Radiology Tree app to read full this article<
MRI and Pharmacokinetic Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Microvessel Density: CD-34 Staining of MM
Get Radiology Tree app to read full this article<
Quantitative Staining Assessment
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Technical Implementation and Pharmacokinetic Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
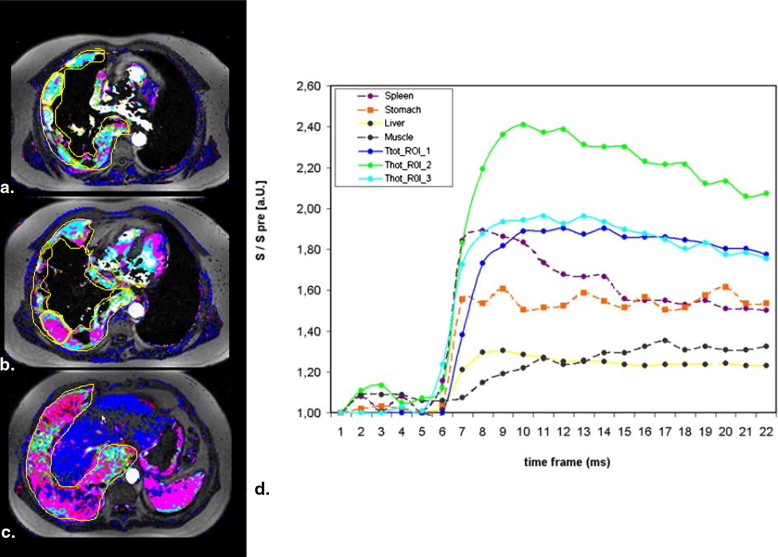
![Figure 3, Pharmacokinetic region of interest (ROI) analysis of the amplitude (inter alia) in different tissue regions (total tumor, hot spot, muscle, spleen, and liver [ n = 19]) are presented. Comparing these different tissue regions can be clearly differentiated from the tumor tissue ( P ≤ .001), apart from the spleen. No statistical differences could be found between tumor hot spot and spleen parenchyma. TT_ROI: total tumor ROI; THot_ROI: tumor hot spot ROI; Tpix_ROI: tumor hotspot one pixel ROI.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/PharmacokineticAnalysisofMalignantPleuralMesotheliomaInitialResultsofTumorMicrocirculationanditsCorrelationtoMicrovesselDensityCD34/2_1s20S1076633207007179.jpg)
Get Radiology Tree app to read full this article<
Microvascular Density by CD-34 Staining
Get Radiology Tree app to read full this article<
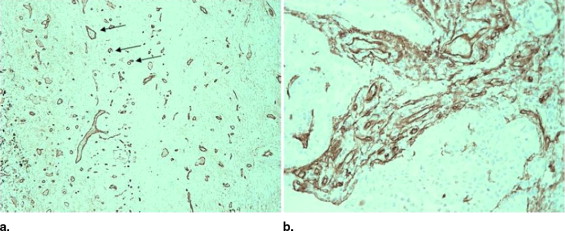
![Figure 5, CD-34 immunohistochemical presentation and automated computerized detection of vessels in a localized fibrous tumors. (Anteroposterior, ×40, segmentation of vascular endothelial cells by Electronic Automated Morphometry User System [EAMUS]). Note the quite large distances between the vessels.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/PharmacokineticAnalysisofMalignantPleuralMesotheliomaInitialResultsofTumorMicrocirculationanditsCorrelationtoMicrovesselDensityCD34/4_1s20S1076633207007179.jpg)
Table 1
Vascular Features of Malignant Epithelial Mesothelioma Obtained by Image Analysis at Light Microscopy Magnification
Counts ( n ) Area (μm 2 ) Circumference (μm) Diffusion Length (μm) Median 53.00 241.0 50.00 31.00 Minimum 18 130 38 13 Maximum 71 737 82 57
Table 2
Comparison of Vascular Features in Malignant Mesotheliomas, LFTs of Pleura, and Primary Lung Carcinomas ( )
Cell Type Number of Cases Diffusion Length (μm) Mean Area (μm 2 ) Mean Circumference (μm) Mesothelioma 19 31 241 50 LFT ⁎ 36 220 105 34 Adeno † 94 27 1765 109 Squamous † 113 29 1803 108 Large cell † 30 22 1901 114 Small cell † 9 22 2091 119
LFT: localized fibrous tumors.
LFTs of the pleura: clinical data, asbestos burden, and syntactic structure analysis applied to newly defined angiogenic/growth regulatory effectors.
In respect to their vascularization, the analyzed tumors form three different, statistically highly significant ( P < .001) cohorts as indicated by (*):
Cohort 1: diffuse epithelial mesotheliomas (small diffusion length, small vascular size).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Correlation of the Pharmacokinetic Parameters and CD-34 Microvascular Staining
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kayser K., Becker C., Seeberg N., et. al.: Quantitation of asbestos and asbestos-like fibers in human lung tissue by hot and wet ashing, and the significance of their presence for survival of lung carcinoma and mesothelioma patients. Lung Cancer 1999; 24: pp. 89-98.
2. Kayser K., Bohm G., Blum S., et. al.: Glyco- and immunohistochemical refinement of the differential diagnosis between mesothelioma and metastatic carcinoma and survival analysis of patients. J Pathol 2001; 193: pp. 175-180.
3. Sugarbaker D.J., Flores R.M., Jaklitsch M.T., et. al.: Resection margins, extrapleural nodal status, and cell type determine postoperative long-term survival in trimodality therapy of malignant pleural mesothelioma: results in 183 patients. J Thorac Cardiovasc Surg 1999; 117: pp. 54-63.
4. Choyke P.L., Dwyer A.J., Knopp M.V.: Functional tumor imaging with dynamic contrast-enhanced magnetic resonance imaging. J Magn Reson Imaging 2003; 17: pp. 509-520.
5. Knopp M.V., Weiss E., Sinn H.P., et. al.: Pathophysiologic basis of contrast enhancement in breast tumors. J Magn Reson Imaging 1999; 10: pp. 260-266.
6. Nosas-Garcia S., Moehler T., Wasser K., et. al.: Dynamic contrast-enhanced MRI for assessing the disease activity of multiple myeloma: a comparative study with histology and clinical markers. J Magn Reson Imaging 2005; 22: pp. 154-162.
7. Hylton N.: Dynamic contrast-enhanced magnetic resonance imaging as an imaging biomarker. J Clin Oncol 2006; 24: pp. 3293-3298.
8. Hawighorst H., Knopp M.V., Debus J., et. al.: Pharmacokinetic MRI for assessment of malignant glioma response to stereotactic radiotherapy: initial results. J Magn Reson Imaging 1998; 8: pp. 783-788.
9. Knopp M.V., Tengg-Kobligk H., Choyke P.L.: Functional magnetic resonance imaging in oncology for diagnosis and therapy monitoring. Mol Cancer Ther 2003; 2: pp. 419-426.
10. Padhani A.R., Gapinski C.J., Macvicar D.A., et. al.: Dynamic contrast enhanced MRI of prostate cancer: correlation with morphology and tumour stage, histological grade and PSA. Clin Radiol 2000; 55: pp. 99-109.
11. Mayr N.A., Hawighorst H., Yuh W.T., et. al.: MR microcirculation assessment in cervical cancer: correlations with histomorphological tumor markers and clinical outcome. J Magn Reson Imaging 1999; 10: pp. 267-276.
12. Butchart E.G., Ashcroft T., Barnsley W.C., et. al.: Pleuropneumonectomy in the management of diffuse malignant mesothelioma of the pleura. Thorax 1976; 31: pp. 15-24.
13. Butchart E.G.: Surgery of mesothelioma of the pleura.Roth J.A.Ruckdeschel J.C.Weinseinberger T.H.Thoracic oncology.1989.WB Saunders CoPhiladelphia, PA:pp. 566-583.
14. Hoffmann U., Brix G., Knopp M.V., et. al.: Pharmacokinetic mapping of the breast: a new method for dynamic MR mammography. Magn Reson Med 1995; 33: pp. 506-514.
15. Brix G., Semmler W., Port R., et. al.: Pharmacokinetic parameters in CNS Gd-DTPA enhanced MR imaging. J Comput Assist Tomogr 1991; 15: pp. 621-628.
16. Kayser K., Trott J., Bohm G., et. al.: Localized fibrous tumors (LFTs) of the pleura: clinical data, asbestos burden, and syntactic structure analysis applied to newly defined angiogenic/growth-regulatory effectors. Pathol Res Pract 2005; 201: pp. 791-801.
17. Kayser K., Gabius H.J.: The application of thermodynamic principles to histochemical and morphometric tissue research: principles and practical outline with focus on the glycosciences. Cell Tissue Res 1999; 296: pp. 443-455.
18. Zou K.H., Tuncali K., Silverman S.G.: Correlation and simple linear regression. Radiology 2003; 227: pp. 617-622.
19. Szoke T., Kayser K., Baumhakel J.D., et. al.: Prognostic significance of microvascularization in cases of operated lung cancer. Eur J Cardiothorac Surg 2005; 27: pp. 1106-1111.
20. Kayser G., Baumhakel J.D., Szoke T., et. al.: Vascular diffusion density and survival of patients with primary lung carcinomas. Virchows Arch 2003; 442: pp. 462-467.
21. Galbraith S.M., Rustin G.J., Lodge M.A., et. al.: Effects of 5,6-dimethylxanthenone-4-acetic acid on human tumor microcirculation assessed by dynamic contrast-enhanced magnetic resonance imaging. J Clin Oncol 2002; 20: pp. 3826-3840.
22. Sorensen A.G.: Magnetic resonance as a cancer imaging biomarker. J Clin Oncol 2006; 24: pp. 3274-3281.
23. Folkman J.: Tumor angiogenesis: therapeutic implications. N Engl J Med 1971; 285: pp. 1182-1186.
24. Martincich L., Montemurro F., De Rosa G., et. al.: Monitoring response to primary chemotherapy in breast cancer using dynamic contrast-enhanced magnetic resonance imaging. Breast Cancer Res Treat 2004; 83: pp. 67-76.
25. Weidner N., Semple J.P., Welch W.R., et. al.: Tumor angiogenesis and metastasis—correlation in invasive breast carcinoma. N Engl J Med 1991; 324: pp. 1-8.
26. Mattern J., Koomagi R., Volm M.: Association of vascular endothelial growth factor expression with intratumoral microvessel density and tumour cell proliferation in human epidermoid lung carcinoma. Br J Cancer 1996; 73: pp. 931-934.
27. Kumar-Singh S., Vermeulen P.B., Weyler J., et. al.: Evaluation of tumour angiogenesis as a prognostic marker in malignant mesothelioma. J Pathol 1997; 182: pp. 211-216.
28. Ohta Y., Shridhar V., Bright R.K., et. al.: VEGF and VEGF type C play an important role in angiogenesis and lymphangiogenesis in human malignant mesothelioma tumours. Br J Cancer 1999; 81: pp. 54-61.