
Rationale and Objectives
We sought to show that phase-sensitive detection and a single-shot technique allow imaging of the heart for detection of myocardial infarction during a single breathhold without adaptation of the inversion time.
Materials and Methods
Thirty-five patients at 2 weeks to 3 months after Q-wave myocardial infarction were examined on a 1.5-T MR system 10 minutes after the administration of a double-dose extravascular contrast agent. In order to determine the optimal inversion recovery time (TI), a TI scout sequence was performed. An IR-turboFlash sequence with optimized TI was used as standard of reference. A phase-sensitive inversion recovery (PSIR) single-shot TrueFISP sequence, which allows imaging of nine slices during one breathhold (TR/TE/FA/BW: 2.2 ms/1.1 ms/60°, 8°/1220 Hz/Px) was used with a nominal TI of 200 ms. Spatial resolution was identical for both techniques: 1.3 mm × 1.8 mm × 8 mm. Infarct volumes, area of infarction on a selected slice, and scan time for imaging delayed contrast enhancement (DCE) were compared.
Results
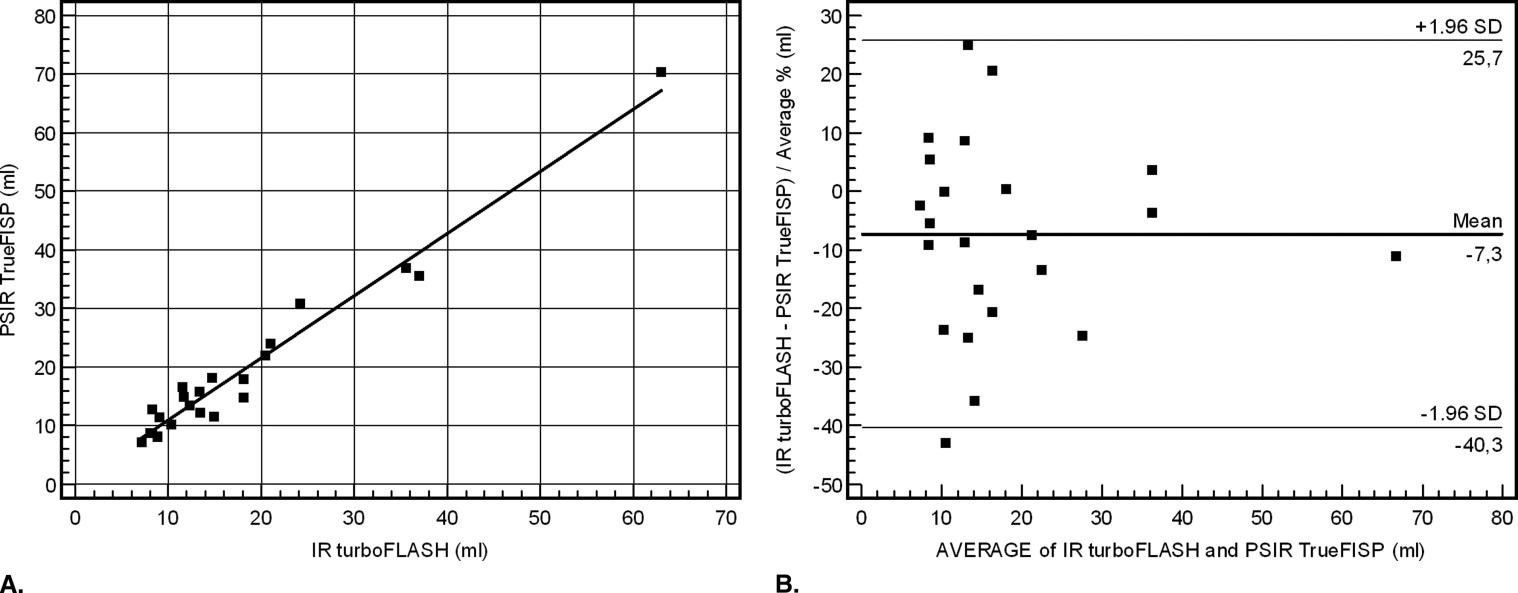
The mean values for the time of imaging DCE were 10 minutes 43 seconds for the IR turboFLASH and 17 seconds ( P < .001) for the PSIR single-shot TrueFISP sequence. No significant difference was found for the mean values of the infarct volumes with 18.7 ml (IR turboFLASH) and 17.3 ml (PSIR single-shot TrueFISP). The values for the correlation coefficients of the infarct volumes and infarct areas of the two different techniques were r = 0.95 ( P < .004) and r = 0.97 ( P < .002). The regression equations were y = 0.76 + 0.92* x and y = 0.07 + 0.93* x , respectively.
Conclusions
PSIR single-shot TrueFISP allows for accurate identification of myocardial infarction during a single breathhold with reduction of scan time by a factor of 38.
Imaging myocardial infarction by MRI using the effect of delayed hyperenhancement is an established and accurate method (1−5). In patients with coronary artery disease and left ventricular dysfunction, the distinction between viable and nonviable myocardium by contrast-enhanced MRI allows the prediction of functional recovery after surgical or interventional revascularization ( ). In contrast to positron-emission tomography and single-photon-emission computed tomography ( ), delayed contrast-enhanced MRI has superior spatial resolution and can differentiate transmural from nontransmural myocardial infarction. The area of hyperenhancement shows a close correlation with histopathologically determined area of myocardial infarction (MI) in animal experiments ( ).
The most widely used pulse sequence type to depict late enhancing areas in the myocardium is inversion-recovery (IR) turboFLASH with magnitude reconstruction. This pulse sequence requires an individual adaptation of the inversion-recovery time (TI) to achieve optimal signal increase between infarcted and viable myocardium. At the optimal TI, the signal intensity of normal myocardium is nulled. Several breathholds can be necessary to determine the optimal TI value. An error in selection of the optimum null time leads to a reduction in contrast and may reduce the visible hyperenhanced area and therefore may cause an underestimation of the extent of the infarction ( ).
Get Radiology Tree app to read full this article<
Materials and methods
Patient Population
Get Radiology Tree app to read full this article<
MRI
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Evaluation
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Kim R.J., Wu E., Rafael A., et. al.: The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med 2000; 343: pp. 1445-1453.
2. Kim R.J., Fieno D.S., Parrish T.B., et. al.: Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation 1999; 100: pp. 1992-2002.
3. Simonetti O.P., Kim R.J., Fieno D.S., et. al.: An improved MR imaging technique for the visualization of myocardial infarction. Radiology 2001; 218: pp. 215-223.
4. Kuhl H.P., Beek A.M., van der Weerdt A.P., et. al.: Myocardial viability in chronic ischemic heart disease: Comparison of contrast-enhanced magnetic resonance imaging with (18) F-fluorodeoxyglucose positron emission tomography. J Am Coll Cardiol 2003; 41: pp. 1341-1348.
5. Kellman P., Arai A.E., McVeigh E.R., Aletras A.H.: Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med 2002; 47: pp. 372-383.
6. Wagner M.H., Holly T.A., Elliot M.D., et. al.: Contrast-enhanced MRI and routine single photon emission comoputed tomography (SPECT) perfusion imaging for detection of subendocardial myocardial infarcts: An imaging study. Lancet 2003; 361: pp. 374-394.
7. Huber A.M., Schoenberg S.O., Hayes C., et. al.: Phase-sensitive inversion-recovery MR imaging in the detection of myocardial infarction. Radiology 2005; 237: pp. 854-860.
8. Li W., Li B.S.Y., Polzin J.A., Mai V.M., Prasad P.V., Edelman R.R.: Myocardial delayed enhancement imaging using inversion recovery single-shot steady-state free precession: initial experience. J Magn Reson Imaging 2004; 20: pp. 327-330.
9. Huber A., Bauner K., Wintersperger B.J., et. al.: Phase-sensitive inversion recovery (PSIR) Single-shot TrueFISP for assessment of myocardial infarction at 3 Tesla. Invest Radiol 2006; 41: pp. 148-153.
10. Huber A., Schoenberg S.O., Spannagl B., Rieber J., Erhard I., Klauss V., Reiser M.F.: Single-shot inversion recovery TrueFISP for assessment of myocardial infarction. Am J Roentgenol 2006; 186: pp. 627-633.
11. Gupta A., Lee V.S., Chung Y.C., Babb J.S., Simonetti O.P.: Myocardial infarction: Optimization of inversion times at delayed contrast-enhanced MR imaging. Radiology 2004; 233: pp. 921-926.
12. Flacke A.J.S., Chia J.M., Wible J.H., Periasamy M.P., Adams M.D., Adzamli I.K., Lorenz C.H.: Characterization of viable and nonviable myocardium at MR imaging: Comparison of gadolinium-based extracellular and blood pool contrast materials versus manganese-based contrast materials in a rat myocardial infarction model. Radiology 2003; 226: pp. 731-738.
13. Klein C., Nekolla S.G., Bengel F.M., et. al.: Assessment of myocardial viability with contrast-enhanced magnetic resonance imaging: Comparison with positron emission tomography. Circulation 2002; 105: pp. 162-167.
14. Bello D., Shah D.J., Farah G.M., et. al.: Gadolinium cardiovascular magnetic resonance predicts reversible myocardial dysfunction and remodeling in patients with heart failure undergoing beta-blocker therapy. Circulation 2003; 108: pp. 1945-1953.
15. Jimenez Borreguero L.J., Ruiz-Salmeron R.: Assessment of myocardial viability in patients before revascularization. Rev Esp Cardiol 2003; 56: pp. 721-733.
16. Noll D.C., Nishimura D.G., Macovski A.: Homodyne detection in magnetic-resonance-imaging. IEEE Trans Med Imaging 1991; 1: pp. 154-163.
17. Higgins C.B., Herfkens R., Lipton M.J., et. al.: Nuclear magnetic resonance imaging of acute myocardial infarction in dogs: Alterations in magnetic relaxation times. Am J Cardiol 1983; 52: pp. 184-188.
18. Oshinski J., Yang Z., Jones J., Mata J., French B.: Imaging time after Gd-DTPA injection is critical in using delayed enhancement to determine infarct size accurately with magnetic resonance imaging. Circulation 2001; 104: pp. 2838-2842.
19. Kellman P., Larson A.C., Hsu L.Y., Chung Y.C., Simonetti O.P., McVeigh E.R., Arai A.E.: Motion-corrected free-breathing delayed enhancement imaging of myocardial infarction. Magn Reson Med 2005; 53: pp. 194-200.
20. Wintersperger B.J., Reeder S.B., Nikolaou K., et. al.: Cardiac CINE MR imaging with a 32-channel cardiac coil and parallel imaging: Impact of acceleration factors on image quality and volumetric accuracy. J Magn Reson Imaging 2006; 23: pp. 222-227.
21. Scheffler K., Henning J.T.: Quantification with inversion recovery TrueFISP. Magn Reson Med 2001; 45: pp. 720-723.