
The availability of the Picture Archiving and Communication System (PACS) has revolutionized the practice of radiology in the past two decades and has shown to eventually increase productivity in radiology and medicine. PACS implementation and integration may bring along numerous unexpected issues, particularly in a large-scale enterprise. To achieve a successful PACS implementation, identifying the critical success and failure factors is essential. This article provides an overview of the process of implementing and integrating PACS in a comprehensive health system comprising an academic core hospital and numerous community hospitals. Important issues are addressed, touching all stages from planning to operation and training. The impact of an enterprise-wide radiology information system and PACS at the academic medical center (four specialty hospitals), in six additional community hospitals, and in all associated outpatient clinics as well as the implications on the productivity and efficiency of the entire enterprise are presented.
Since the emergence of a Picture Archiving and Communication System (PACS) in the early 1980s, we have witnessed revolutionary changes in radiology practice. Early years mostly dealt with the definition of large scale PACS, establishment of Digital Imaging and Communications in Medicine (DICOM) and other standards, the development of some early key PACS-related technologies, and PACS implementation strategies. Concepts such as enterprise PACS, integrating the health care enterprise workflow profiles, and EMR (electronic medical records) with image distribution were developed later . In 1995 Bauman et al conducted a worldwide survey of 82 institutions to investigate the number of large-scale installations and found an increase from 13 to 23 within 15 months, and they concluded there was a strong trend toward filmless radiology throughout the world . At the time, Bauman et al defined large-scale PACS by four criteria: 1) daily active clinical operation; 2) covering at least three modalities; 3) including workstations inside and outside of the radiology department; and 4) performing more than 20,000 examinations annually . In 1996 Huang et al described various types of PACS designs and styles of implementation and illustrated the gradual transition in hospitals from closed architectures to open integrated systems comprising multiple advanced technology components linked through stable digital interfaces . Eventually, between 2000 and 2005, guidelines for PACS installation were developed to outline structure and optimize the implementation process . Since the original PACS environments, users have faced growing demands for increased and more complex integration with other hospital systems beginning with a radiology information system (RIS). The increasing demand for communication of radiology information then expanded to systems outside radiology and ultimately to clinical integration of PACS into a larger organizational body of live clinical systems including the Hospital Information System (HIS) and EMR, with emphasis on integration of images into the overall workflow and record . After the implementation and integration, there remains a sustained requirement for a systematic process to establish and maintain the functionality of the system with training specific to the needs of users. Ongoing training and continued train-the-trainer concepts are representative of areas needing meticulous attention before and after the PACS implementation .
After completion of a complex integrated PACS implementation with successful training, one will encounter changes to clinical care reflected in workflow, clinical productivity, and system efficiency. In the early 1990s, different financial models were defined to analyze and justify the cost-effectiveness of PACS ; however, subsequently and especially after large PACS installation, there are increasing demands to evaluate the financial implications of the implementation. The most important parameters that have been studied are: reducing the number of unread, retaken, and lost films; increasing productivity; and reducing turnaround time . In 2009 Ayal et al published a comprehensive article on the financial objective of integrating EMR with the RIS and PACS at their medical center . They analyzed the impact of enterprise information systems at a large-scale service organization reviewing measurements of financial revenues, operating lead times, clinical process lead time, and subjective satisfaction levels by radiology staff and physicians. These measurements showed that, for the subsequent 12 months after installation, these performance measures kept improving at the rate of 63% .
In this article, we offer a review of a PACS implementation and integration in a current large-scale health system enterprise across an integrated hospital delivery network. The components around an implementation including integration, testing and support are described, then specifics of our implementation are presented, and finally improvements in productivity and efficiency as well as challenges and problems encountered are detailed.
Preparation for implementation
Contract
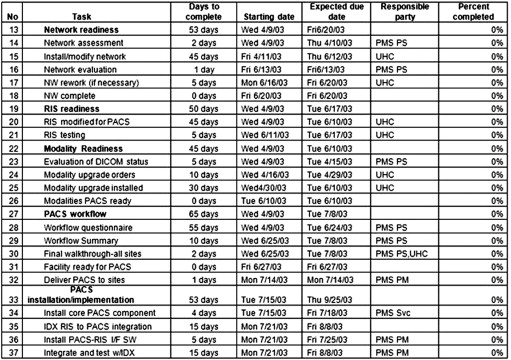
In developing a PACS contract, it is essential to agree not only on the financial terms, but also agree to milestones and to specify each party’s responsibilities . First, a detailed discussion of work plans is needed so buyers and vendors can mutually target the expected dates of completion. Though every date may not be predetermined during negotiation, the overall length of time necessary must be noted with sufficient dates for standardized work plan templates to delineate tasks for each side ( Fig 1 ). Second, penalties for delayed installations, unscheduled downtime, and failure to achieve performance measures should be defined. Third, agreements should be obtained for vendor support on interfaces, integration, and maintenance with services including repairs or upgrades during the life of the contract is clearly defined and additional costs and fees are predetermined.
Team
Get Radiology Tree app to read full this article<
Site-specific Information
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Initiation of implementation
Network
Get Radiology Tree app to read full this article<
Construction
Get Radiology Tree app to read full this article<
Integration
Get Radiology Tree app to read full this article<
Testing
Get Radiology Tree app to read full this article<
Training
Get Radiology Tree app to read full this article<
Security
Get Radiology Tree app to read full this article<
Going Live
Get Radiology Tree app to read full this article<
After implementation
Get Radiology Tree app to read full this article<
PACS solution in an integrated health care system: university hospitals
Get Radiology Tree app to read full this article<
UH PACS Implementation
Get Radiology Tree app to read full this article<
Current PACS at UH
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Business objectives of PACS implementation at UH
Get Radiology Tree app to read full this article<
Improvement in Physician Productivity Indicators
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Reduce Turnaround Time for Report Dictation
Get Radiology Tree app to read full this article<
Eliminating Film-related Costs
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Labor Expenses Reductions
Get Radiology Tree app to read full this article<
Challenges encountered during and after PACS implementation
Get Radiology Tree app to read full this article<
Networking
Get Radiology Tree app to read full this article<
User Acceptance and Communication
Get Radiology Tree app to read full this article<
Vendor Compliance
Get Radiology Tree app to read full this article<
Future PACS horizons
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Huang H.K.: Short history of PACS. Part 1: USA. Eur J Radiol 2011; 78: pp. 163-176.
2. Bauman R.A., Gell G., Dwyer S.J.: Large picture archiving and communication systems of the world—Part 1. J Digit Imaging 1996; 9: pp. 99-103.
3. Huang H.K., Andriole K., Bazzill T., et. al.: Design and implementation of a picture archiving and communication system: the second time. J Digit Imaging 1996; 9: pp. 47-59.
4. Pilling J.R.: Lessons learned from a whole hospital PACS installation. Picture Archiving and Communication System. Clin Radiol 2002; 57: pp. 784-788.
5. Hirschorn D., Eber C., Samuels P., et. al.: Filmless in New Jersey: the New Jersey Medical School PACS Project. J Digit Imaging 2002; 15: pp. 7-12.
6. Carrino J.A., Unkel P.J., Miller I.D., et. al.: Large-scale PACS implementation. J Digit Imaging 1998; 11: pp. 3-7.
7. De Backer A.I., Mortelé K.J., De Keulenaer B.L.: Picture archiving and communication system—considerations for planning and implementation. JBR-BTR 2004; 87: pp. 241-246.
8. vanEssen J., Hough T.: An overview of a picture archiving and communications system procurement. J Digit Imaging 2001; 14: pp. 34-39.
9. Bellon E., Feron M., Deprez T., et. al.: Integrating images into a central medical information system. Stud Health Technol Inform 2002; 93: pp. 53-60.
10. Kotter E., Langer M.: Integrating HIS-RIS-PACS: the Freiburg experience. Eur Radiol 1998; 8: pp. 1707-1718.
11. Honea R., Mensch B.: Maintaining continuity of clinical operations while implementing large-scale filmless operations. J Digit Imaging 1999; 12: pp. 50-53.
12. Blado M.E., Carr S.G.: PACS training modules at Texas Children’s Hospital. J Digit Imaging 2004; 17: pp. 124-133.
13. Hilsenrath P.E., Smith W.L., Berbaum K.S., et. al.: Analysis of the cost effectiveness of PACS. AJR Am J Roentgenol 1991; 156: pp. 177-180.
14. Becker S.H., Arenson R.L.: Costs and benefits of picture archiving and communication systems. J Am Med Inform Assoc 1994; 1: pp. 361-371.
15. Strickland N.H.: Review article: some cost-benefit considerations for PACS: a radiological perspective. Br J Radiol 1996; 69: pp. 1089-1098.
16. Fang Y.C., Yang M.C., Hsueh Y.S.: Financial assessment of a picture archiving and communication system implemented all at once. J Digit Imaging 2006; 19: pp. 44-51.
17. Ayal M., Seidmann A.: An empirical investigation of the value of integrating enterprise information systems: the case of medical imaging informatics. J Manage Inform Sys 2009; 26: pp. 43-68.
18. Birjandi A.: Essentials of a good RIS/PACS contract. Following the rules of engagement in negotiating a partnership can prevent surprises or disappointments in a RIS/PACS implementation. Health Manage Technol 2004; 25: pp. 34-37.
19. Breant C.M., Taira R.K., Huang H.K.: Interfacing aspects between the picture archiving communications systems, radiology information systems, and hospital information systems. J Digit Imaging 1993; 6: pp. 88-94.
20. Huang H.K.: From PACS to web-based ePR system with image distribution for enterprise-level filmless healthcare delivery. Radiol Phys Technol 2011; 4: pp. 91-108.
21. Cohen M.D., Rumreich L.L., Garriot K.M., et. al.: Planning for PACS: a comprehensive guide to nontechnical considerations. J Am Coll Radiol 2005; 2: pp. 327-337.
22. University hospitals. About UH. Available at: http://www.uhhospitals.org/AboutUH.aspx . Accessed September 25, 2011.
23. University Hospitals Seidman Cancer Center. Available at: http://www.uhhospitals.org/irelandcancer/AboutUs.aspx . Accessed September 25, 2011.
24. University Hospitals Ahuja Medical Center. Available at: http://www.uhhospitals.org/aboutuh/vision2010theuhdifference/tabid/2306/uhahujamedicalcenter.aspx . Accessed September 25, 2011.
25. Top national hospitals. Available at: http://www.100tophospitals.com/top-national-hospitals/index.html#winners . Accessed September 25, 2011.
26. Lepanto L., Paré G., Gauvin A.: Impact of PACS deployment strategy on dictation turnaround time of chest radiographs. Acad Radiol 2006; 13: pp. 447-452.
27. Reiner B.I., Siegel E.L., Hooper F.J., et. al.: Effect of film-based versus filmless operation on the productivity of CT technologists. Radiology 1998; 207: pp. 481-485.
28. Chan L., Trambert M., Kywi A., et. al.: PACS in private practice-effect on profits and productivity. J Digit Imaging 2002; 15: pp. 131-136.
29. Reiner B.I., Siegel E.L.: Technologists’ productivity when using PACS: comparison of film-based versus filmless radiography. AJR Am J Roentgenol 2002; 179: pp. 33-37.
30. Sferrella S.M.: Success with voice recognition. Radiol Manage 2003; 25: pp. 42-49.
31. Krishnaraj A., Lee J.K., Laws S.A., et. al.: Voice recognition software: effect on radiology report turnaround time at an academic medical center. AJR Am J Roentgenol 2010; 195: pp. 194-197.
32. De Backer A.I., Mortelé K.J., De Keulenaer B.L.: Picture archiving and communication system-part 2 cost-benefit considerations for picture archiving and communication system. JBR-BTR 2004; 87: pp. 296-299.
33. Bick U., Lenzen H.: PACS: the silent revolution. Eur Radiol 1999; 9: pp. 1152-1160.
34. Maass M., Kosonen M., Kormano M.: Cost analysis of Turku University Central Hospital PACS in 1998. Comput Methods Programs Biomed 2001; 66: pp. 41-45.