
Rationale and Objectives
The human lung and its functions are extremely sensitive to orientation and posture, and debate continues as to the role of gravity and the surrounding anatomy in determining lung function and heterogeneity of perfusion and ventilation. However, study of these effects is difficult. The conventional high-field magnets used for most hyperpolarized 3 He magnetic resonance imaging (MRI) of the human lung, and most other common radiologic imaging modalities including positron emission tomography and computed tomography, restrict subjects to lying horizontally, minimizing most gravitational effects.
Materials and Methods
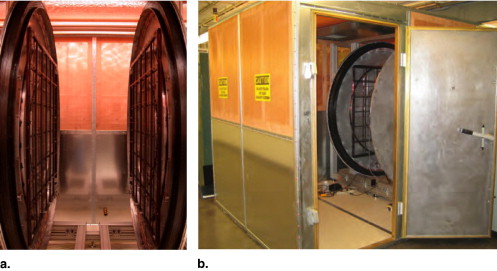
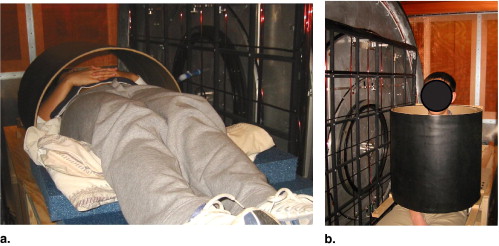
In this article, we review the motivation for posture-dependent studies of human lung function and present initial imaging results of human lungs in the supine and vertical body orientations using inhaled hyperpolarized 3 He gas and an open-access MRI instrument. The open geometry of this MRI system features a “walk-in” capability that permits subjects to be imaged in vertical and horizontal positions and potentially allows for complete rotation of the orientation of the imaging subject in a two-dimensional plane.
Results
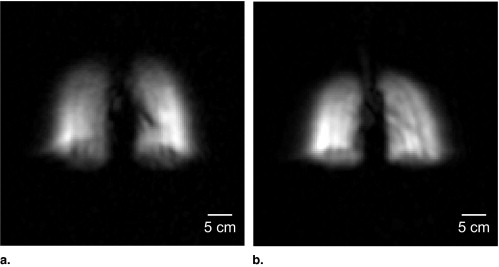
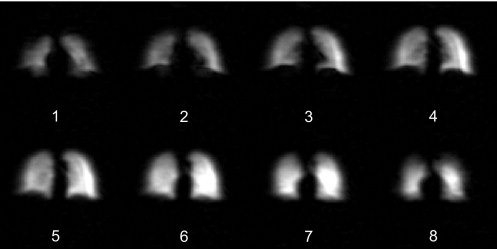
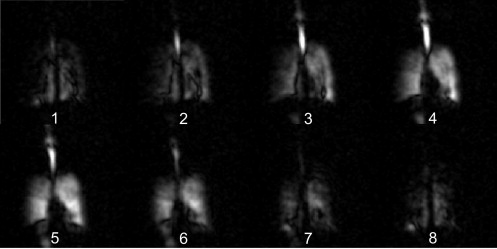
Initial results include two-dimensional lung images acquired with ∼4 × 8 mm in-plane resolution and three-dimensional images with ∼2-cm slice thickness.
Conclusions
Effects of posture variation are observed, including posture-related effects of the diaphragm and distension of the lungs while vertical.
The effects of body orientation and posture changes on the regional distribution of pulmonary perfusion and ventilation have been a source of renewed interest in recent years ( ), principally because of significant questions relating to the care and survival of patients with obstructive or restrictive lung diseases such as acute respiratory distress syndrome ( ). Perfusion heterogeneity has classically been attributed to effects of gravity on pleural pressure and alveolar expansion, resulting in regional variations in lung function ( ). Position-dependent changes in ventilation dynamics also play an important role in a variety of common clinical problems ( ). Few methods exist that allow detailed studies of regional lung function under varying gravitational conditions—or subject orientations. Thus pulmonary physiology could benefit greatly from the development of minimally invasive methods to quantify regional lung function in subjects at variable orientations.
Magnetic resonance imaging (MRI) has only recently been recognized as a useful tool for pulmonary imaging. Chest radiography ( ) offers rapid, low-cost, high-resolution projection images with multiple subject orientations, but yields no quantitative information on gas exchange. Scintigraphy ( ) offers tomographic and quantitative information but uses relatively high and costly doses of nuclear tracers and suffers from poor resolution. Computed tomography provides superior anatomic detail with limited functional data ( ). Positron emission tomography (PET) and PET/computed tomography are used to directly measure pulmonary ventilation and perfusion and have provided the best regional quantitative detail thus far ( ), but subjects are restricted to prone or supine orientations.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Background
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Experimental
Imager Design
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MRI Techniques
Get Radiology Tree app to read full this article<
Polarized 3 He Production and Delivery
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Human Imaging Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results and discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Mure M., Domino K.B., Lindahl S.G.E., et. al.: Regional ventilation-perfusion distribution is more uniform in the prone position. J Appl Physiol 2000; 88: pp. 1076-1083.
2. Mure M., Lindahl S.G.E.: Prone position improves gas exchange—but how?. Acta Anaesthesiol Scand 2001; 45: pp. 150-159.
3. Gattinoni L., Tognoni G., Pesenti A., et. al.: Effect of prone positioning on the survival of patients with acute respiratory failure. N Engl J Med 2001; 345: pp. 568-573.
4. Musch G., Layfield J.D., Harris R.S., et. al.: Topographical distribution of pulmonary perfusion and ventilation, assessed by PET in supine and prone humans. J Appl Physiol 2002; 93: pp. 1841-1851.
5. Glenny R.W., Lamm W.J., Albert R.K., et. al.: Gravity is a minor determinant of pulmonary blood flow distribution. J Appl Physiol 1991; 71: pp. 620-629.
6. West J.B., Hlastala M.P.: Importance of gravity in determining the distribution of pulmonary blood flow. J Appl Physiol 2002; 93: pp. 1888-1891.
7. Fahy B.G., Barnas G.M., Nagle S.E., et. al.: Effects of Trendelenburg and reverse Trendelenburg postures on lung and chest wall mechanics. J Clin Anesth 1996; 8: pp. 236-244.
8. Yap J.C., Watson R.A., Gilbey S., et. al.: Effects of posture on respiratory mechanics in obesity. J Appl Physiol 1995; 79: pp. 1199-1205.
9. Watson R.A., Pride R.B.: Postural changes in lung volumes and respiratory resistance in subjects with obesity. J Appl Physiol 2005; 98: pp. 512-517.
10. Potchen E.J., Cooper T.G., Sierra A.E., et. al.: Measuring performance in chest radiography. Radiology 2000; 217: pp. 456-459.
11. Taplin G.V., Poe N.D.: A dual lung-scanning technique for evaluation of pulmonary function. Radiology 1965; 85: pp. 365-368.
12. Mayo J.R., Webb W.R., Gould R., et. al.: High-resolution CT of the lungs—an optimal approach. Radiology 1987; 163: pp. 507-510.
13. Jones A.R., Hansell D.M., Evans T.W.: Pulmonary perfusion in supine and prone positions: an electron-beam computed tomography study. J Appl Physiol 2001; 90: pp. 1342-1348.
14. Saba O.I., Chon D., Beck K., et. al.: Static versus prospective gated non–breath hold volumetric MDCT imaging of the lungs. Acad Radiol 2005; 12: pp. 1371-1384.
15. Layfield D., Venegas J.G.: Enhanced parameter estimation from noisy PET data: part I—methodology. Acad Radiol 2005; 12: pp. 1440-1447.
16. Walker T.G., Happer W.: Spin-exchange optical pumping of noble-gas nuclei. Rev Mod Phys 1997; 69: pp. 629-642.
17. Nacher P.J., Leduc M.: Optical pumping in 3 He with a laser. J Physique 1985; 46: pp. 2057-2073.
18. Leawoods J.C., Yablonskiy D.A., Saam B., et. al.: Hyperpolarized 3 He gas production and MR imaging of the lung. Concepts Magn Reson 2001; 13: pp. 277-293.
19. Moller H.E., Chen X.J., Saam B., et. al.: MRI of the lungs using hyperpolarized noble gases. Magn Reson Med 2002; 47: pp. 1029-1051.
20. Salerno M., de Lange E.E., Altes T.A., et. al.: Emphysema: hyperpolarized helium 3 diffusion MR imaging of the lungs compared with spirometric indexes—initial experience. Radiology 2002; 222: pp. 252-260.
21. Saam B.T., Yablonskiy D.A., Kodibagkar V.D., et. al.: MR imaging of diffusion of 3 He gas in healthy and diseased lungs. Magn Reson Med 2000; 44: pp. 174-179.
22. Deninger A.J., Eberle B., Ebert M., et. al.: He-3-MRI-based measurements of intrapulmonary p(O 2 ) and its time course during apnea in healthy volunteers: first results, reproducibility, and technical limitations. NMR Biomed 2000; 13: pp. 194-201.
23. Rizi R.R., Baumgardner J.E., Ishii M., et. al.: Determination of regional V A /Q by hyperpolarized 3 He MRI. Magn Reson Med 2004; 52: pp. 65-72.
24. Mills G.H., Wild J.M., Eberle B., et. al.: Functional magnetic resonance imaging of the lung. BJA: Brit J Anaesth 2003; 91: pp. 16-30.
25. Altes T.A., Powers P.L., Knight-Scott J., et. al.: Hyperpolarized 3 He MR lung ventilation imaging in asthmatics: preliminary findings. J Magn Reson Imag 2001; 13: pp. 378-384.
26. Samee S., T , Altes T.A., Powers P., et. al.: Imaging the lungs in asthmatic patients by using hyperpolarized helium-3 magnetic resonance: assessment of response to methacholine and exercise challenge. J Allergy Clin Immunol 2003; 111: pp. 1205-1211.
27. Kauczor H.U., Ebert M., Kreitner K.F., et. al.: Imaging of the lungs using 3 He MRI: preliminary clinical experience in 18 patients with and without lung disease. J Magn Reson Imaging 1997; 7: pp. 538-543.
28. de Lange E.E., Mugler J.P., Brookeman J.R., et. al.: Lung air spaces: MR imaging evaluation with hyperpolarized 3 He gas. Radiology 1999; 210: pp. 851-857.
29. Donnelly L.F., MacFall J.F., McAdams H.P., et. al.: Cystic fibrosis: combined hyperpolarized 3He-enhanced and conventional proton MR imaging in the lung-preliminary observations. Radiology 1999; 212: pp. 885-889.
30. Guenther D., Eberle B., Hast J., et. al.: 3 He MRI in healthy volunteers: preliminary correlation with smoking history and lung volumes. NMR Biomed 2000; 13: pp. 182-189.
31. Fichele S., Woodhouse N., Swift A.J., et. al.: MRI of helium-3 gas in healthy lungs: posture related variations of alveolar size. J Magn Reson Imag 2004; 20: pp. 331-335.
32. Jinkins J.R., Dworkin J.S., Green A.C., et. al.: Upright, weight-bearing, dynamic-kinetic MRI of the spine pMRI/kMRI. Rivista Neuroradiol 2002; 15: pp. 333-356.
33. Jinkins J.R., Dworkin J.S., Green A.C., et. al.: Upright, weight-bearing, dynamic-kinetic magnetic resonance imaging of the spine review of the first clinical results. Rivista Neuroradiol 2003; 16: pp. 55-74.
34. Jinkins J.R., Dworkin J.S., Damadian R.V.: Upright, weight-bearing, dynamic-kinetic MRI of the spine: initial results. Eur Radiol 2005; 15: pp. 1815-1825.
35. Tseng C.H., Wong G.P., Pomeroy V.R., et. al.: Low-field MRI of laser polarized noble gas. Phys Rev Lett 1998; 81: pp. 3785-3788.
36. Wong G.P., Tseng C.H., Pomeroy V.R., et. al.: A system for low field imaging of laser-polarized noble gas. J Magn Reson 1999; 141: pp. 217-227.
37. Mair R.W., Hrovat M.I., Patz S., et. al.: 3 He lung imaging in an open access, very-low-field human magnetic resonance imaging system. Magn Reson Med 2005; 53: pp. 745-749.
38. Ruset I.C., Tsai L.L., Mair R.W., et. al.: A system for open-access He-3 human lung imaging at very low field. Concepts Magn Reson B Magn Reson Eng 2006; 29B: pp. 210-221.
39. Parra-Robles J., Cross A.R., Santyr G.E.: Theoretical signal-to-noise ratio and spatial resolution dependence on the magnetic field strength for hyperpolarized noble gas magnetic resonance imaging of human lungs. Med Phys 2005; 32: pp. 221-229.
40. Durand E., Guillot G., Darrasse L., et. al.: CPMG measurements and ultrafast imaging in human lungs with hyperpolarized helium-3 at low field (0.1 T). Magn Reson Med 2002; 47: pp. 75-81.
41. Owers-Bradley J.R., Fichele S., Bennattayalah A., et. al.: MR tagging of human lungs using hyperpolarized He-3 gas. J Magn Reson Imaging 2003; 17: pp. 142-146.
42. Venkatesh A.K., Zhang A.X., Mansour J., et. al.: MRI of the lung gas-space at very low-field using hyperpolarized noble gases. Magn Reson Imaging 2003; 21: pp. 773-776.
43. Bidinosti C.P., Choukeife J., Nacher P.J., et. al.: In vivo NMR of hyperpolarized 3 He in the human lung at very low magnetic fields. J Magn Reson 2003; 162: pp. 122-132.
44. Bidinosti C.P., Choukeife J., Tastevin G., et. al.: MRI of the lung using hyperpolarized 3 He at very low magnetic field (3 mT). Magma 2004; 16: pp. 255-258.
45. West J.B., Dollery C.T., Naimark A.: Distribution of blood flow in isolated lung; relation to vascular and alveolar pressures. J Appl Physiol 1964; 19: pp. 713-724.
46. Frerichs I., Dudykevych T., Hinz J., et. al.: Gravity effects on regional lung ventilation determined by functional EIT during parabolic flights. J Appl Physiol 2001; 91: pp. 39-50.
47. Williams M.D., Murr P.C.: Laparoscopic insufflation of the abdomen depresses cardiopulmonary function. Surg Endosc 1993; 7: pp. 12-16.
48. Druz W.S., Sharp J.T.: Activity of respiratory muscles in upright and recumbent humans. J Appl Physiol 1981; 51: pp. 1552-1561.
49. Behrakis P.K., Baydur A., Jaeger M.J., et. al.: Lung mechanics in sitting and horizontal body positions. Chest 1983; 83: pp. 643-646.
50. Barnas G.M., Green M.D., Mackenzie C.F., et. al.: Effect of posture on lung and regional chest wall mechanics. Anesthesiology 1993; 78: pp. 251-259.
51. Kolarzyk E., Szot W.M., Lyszczarz J.: Lung function and breathing regulation parameters during pregnancy. Arch Gynecol Obstet 2005; 272: pp. 53-58.
52. Fischer M.C., Kadlecek S., Yu J., et. al.: Measurements of regional alveolar oxygen pressure using hyperpolarized 3 He MRI. Acad Radiol 2000; 12: pp. 1430-1439.
53. Vidal Melo M.F., Layfield D., Harris R.S., et. al.: Quantification of regional ventilation-perfusion ratios with PET. J Nucl Med 2003; 44: pp. 1982-1991.
54. Rhodes C.G., Valind S.O., Brudin L.H., et. al.: Quantification of regional V/Q ratios in humans by use of PET. J Appl Physiol 1989; 66: pp. 1896-1904.
55. Rhodes C.G., Valind S.O., Brudin L.H., et. al.: Quantification of regional V/Q ratios in humans by use of PET. J Appl Physiol 1989; 66: pp. 1905-1913.
56. Tulic M.K., Christodoulopoulos P., Hamid Q.: Small airway inflammation in asthma. Respir Res 2001; 2: pp. 333-339.
57. Hamid Q.A.: Peripheral inflammation is more important than central inflammation. Respir Med 1997; 91: pp. 11-12.
58. Hamid Q., Song Y.L., Kotsimbos T.C., et. al.: Inflammation of small airways in asthma. J Allergy Clin Immunol 1997; 100: pp. 44-51.
59. Poutler L.W.: Central inflammation is more important than peripheral inflammation. Respir Med 1997; 91: pp. 9-10.
60. Shaw R.J., Djukanovic R., Tashkin D.P., et. al.: The role of small airways in lung disease. Respir Med 2002; 96: pp. 67-80.
61. Venegas J.G., Winkler T., Musch G., et. al.: Self-organized patchiness in asthma as a prelude to catastrophic shifts. Nature 2005; 434: pp. 777-782.
62. Chan E.D., Welsh C.H.: Geriatric respiratory medicine. Chest 1998; 114: pp. 1704-1733.
63. Johnson B.D., Reddan W.G., Pegelow D.F., et. al.: Flow limitation and regulation of functional residual capacity during exercise in a physically active aging population. Am Rev Respir Dis 1991; 143: pp. 960-967.
64. Hazzard W.R.: Principles of geriatric medicine and gerontology, 5th ed.2003.McGraw-Hill ProfessionalNew York, NY
65. enhamou D., Muir J.F., Melen B.: Mechanical ventilation in elderly patients. Monaldi Arch Chest Dis 1998; 53: pp. 547-551.
66. Barst R.J., McGoon M., Torbicki A., et. al.: Diagnosis and differential assessment of pulmonary arterial hypertension. J Am Coll Cardiol 2004; 43: pp. 40S.
67. Fedullo P.F., Auger W.R., Kerr K.M., et. al.: Chronic thromboembolic pulmonary hypertension. N Engl J Med 2001; 345: pp. 1465-1472.
68. Fedullo P.F., Auger W.R., Moser K.M., et. al.: Hemodynamic response to exercise in patients with chronic, major vessel thromboembolic pulmonary hypertension. Am Rev Respir Dis 1990; 141: pp. A890.
69. Tsai LL, Mair RW, Rosen MS, et al. An open-access, very-low-field MRI system for posture-dependent 3 He human lung imaging. J Magn Reson. In press.
70. Morgan P.S., Conolly S., Mazovski A.: Design of uniform field biplanar magnets. Proc 5th Meeting ISMRM 1997; pp. 1447.
71. Yablonskiy D.A., Sukstanskii A.L., Ackerman J.J.H.: Image artifacts in very low magnetic field MRI: The role of concomitant gradients. J Magn Reson 2005; 174: pp. 279-286.
72. Zhao L., Mulkern R., Tseng C.H., et. al.: Gradient echo imaging considerations for hyperpolarized 129 Xe MR. J Magn Reson B 1996; 113: pp. 179-183.
73. Kim Y.R., Rebro K.J., Schmainda K.M.: Water exchange and inflow affect the accuracy of T1-GRE blood volume measurements: implications for the evaluation of tumor angiogenesis. Magn Reson Med 2002; 47: pp. 1110-1120.
74. Wild J.M., Woodhouse N., Paley M.N.J., et. al.: Comparison between 2D and 3D gradient-echo sequences for MRI of human lung ventilation with hyperpolarized 3 He. Magn Reson Med 2004; 52: pp. 673-678.
75. Wild J.M., Fichele S., Woodhouse N., et. al.: 3D volume-localized pO 2 measurement in the human lung with 3 He MRI. Magn Reson Med 2005; 53: pp. 1055-1064.
76. Kadlecek S.J., Emami K., Fischer M.C., et. al.: Imaging physiological parameters with hyperpolarized gas MRI. Prog Nucl Magn Reson Spectrosc 2005; 47: pp. 187-212.
77. Callaghan P.T.: Principles of Nuclear magnetic resonance microscopy.1991.Oxford University PressOxford, UK