
Rationale and Objectives
The purpose of this study was to design an optimized heart rate (HR)-dependent electrocardiogram (ECG) pulsing protocol for computed tomography coronary angiography (CTCA) on a 256-slice CT scanner and to assess its potential dose reduction retrospectively, based on the retrospective ECG gating data without dose modulation.
Materials and Methods
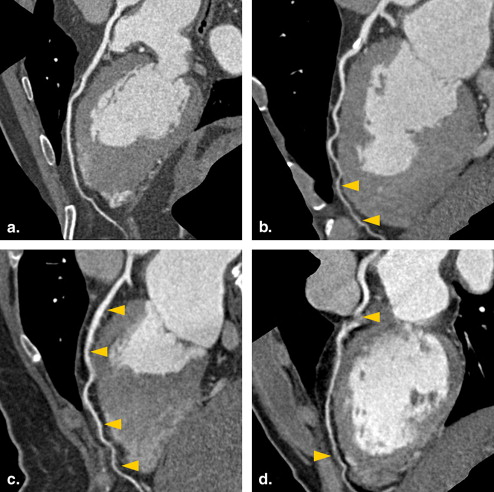
A total of 137 patients were enrolled to perform CTCA with a 256-slice scanner. Two independent radiologists graded image quality of coronary artery segments (1 = excellent, no motion artifacts; 4 = poor, severe motion artifacts) to define optimal reconstruction window in end-systolic phase, mid-diastolic phase, and the combination of both cardiac phases. According to statistical analysis for HR against image quality, four HR-depended ECG-pulsing protocols were proposed. We also demonstrated the potential dose reduction of the proposed technique.
Results
For patients with HR <59 beats/min (group 1), 60–72 beats/min (group 2), 73–84 beats/min (group 3), and >85 beats/min (group 4), the optimal reconstruction windows were at 74.1–81.3%, 73.4–82.2%, 38.3–82.3%, and 37.2–61.6% of R-R interval, respectively. The ECG-pulsing protocols with minimal radiation dose (ie, no tube current outside the pulsing window) can reduce the effective dose of CTCA by 79.5%, 75.7%, 38.3%, and 57.4% for HR groups 1 to 4, respectively. The corresponding results for reducing tube current by 80% outside the pulsing window were 63.7%, 56.6%, 32.0%, and 46.0%.
Conclusion
Through the optimization of ECG-pulsed tube-current modulation, radiation exposure can be greatly reduced, especially in patients with HR <72 beats/min or >85 beats/min.
Computed tomography coronary angiography (CTCA) is highly accurate compared to invasive diagnostic catheterization . Various dose reduction techniques were introduced in CTCA to reduce exposure by approximately 25%–50% . A tube current modulation technique where the x-ray tube is turned on at predefined time points is called prospective electrocardiogram (ECG) triggering. Scheffel et al reported a mean effective dose range of 1.4–4.4 mSv for patients having heart rate (HR) range of 44–69 beats/min . Though this protocol can be applied to a limited number of sporadic arrhythmias , it is usually feasible for patients with monotonous cardiac rhythm and minimal heart rate variability (HRV). Another important strategy for dose reduction in CTCA is ECG-controlled tube current modulation (ETCM) . The tube current is only at maximum within the most quiescent phase of the cardiac cycle, whereas it can be reduced by 80% or more outside the pulsing window, depending if functional evaluation such as valve motion, wall motion or ejection fraction is desirable or not. A study of a dual-source 64-slice CT reported that mean effective dose of 33.4 mSv from CTCA without ETCM can be reduced to 11.0 mSv and 6.8 mSv when tube currents were set at 20% and 4% of the nominal value outside the pulsing window, respectively .
Radiation exposure of CTCA with ETCM technique on 64-slice and dual-source scanners has been investigated in several studies that demonstrated that an effective implementation of ETCM technique is highly dependent on the HR of patients and the temporal resolution of CT scanner. The recently introduced 256-slice CT offers temporal resolutions with a minimum of 135 ms. This scanner also provides z-axial coverage of 80 mm, allowing an acquisition time for the whole heart as low as 5 seconds for a 120-mm z-axial coverage . To the best of our knowledge, no similar study for a 256-slice multidetector CT (MDCT) has been reported yet. The purpose of this study was to design and implement an optimal ECG-pulsing protocol for a 256-slice CT scanner, and evaluate its potential in radiation dose reduction.
Materials and methods
Patient Population
Get Radiology Tree app to read full this article<
CT Acquisition Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Data Postprocessing and Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Radiation Dose
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Overall Image Quality of Optimal Reconstructions in Systolic Phase (S), Diastolic Phase (D), and Combined Systolic and Diastolic Phases (S+D)
Best Image Obtained in S D S+D No. of segments 1800 1800 1800 Overall image quality 1.8 ± 0.5 1.8 ± 0.3 1.5 ± 0.4 Score 1 (%) ∗ 31.6 (569/1800) 38.1 (686/1800) 51.2 (922/1800) Score 2 (%) 58.6 (1055/1800) 49.8 (896/1800) 47.2 (850/1800) Score 3 (%) 9.8 (176/1800) 10.7 (192/1800) 1.6 (28/1800) Score 4 (%) 0.0 (0/1800) 1.4 (26/1800) 0.0 (0/1800)
Get Radiology Tree app to read full this article<
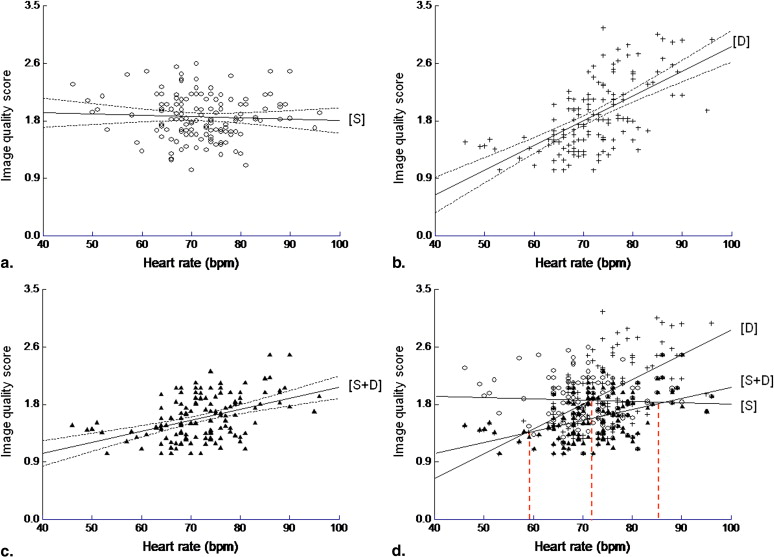
Table 2
Demographic Data of Patients in Four HR Groups
Characteristic HR ≤59 beats/min HR 60–72 beats/min HR 73–84 beats/min HR ≥85 beats/min No. of patients 10 59 57 11 Age (y) 68.3 ± 9.5 55.7 ± 10.6 55.9 ± 8.5 60.3 ± 6.9 Female/male 3/7 15/44 29/28 4/7 Body mass index (kg/m 2 ) 26.1 ± 3.4 26.4 ± 4.4 24.7 ± 3.3 25.8 ± 3.5 Average heart rate (beats/min) 57.3 ± 2.5 67.3 ± 2.7 76.3 ± 3.1 87.2 ± 1.9 Heart rate variability (beats/min) 1.2 ± 0.2 1.4 ± 0.8 1.3 ± 0.6 1.0 ± 0.5 Scan length (mm) 129.6 ± 13.3 131.3 ± 13.6 128.7 ± 13.5 127.0 ± 16.2 Scan time (seconds) 4.6 ± 0.6 4.9 ± 0.3 5.0 ± 0.3 5.0 ± 0.5 CTDI vol (mGy) 66.8 ± 11.2 61.0 ± 12.1 58.8 ± 8.8 57.1 ± 4.7
CTDI vol , volume computed tomography dose index.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
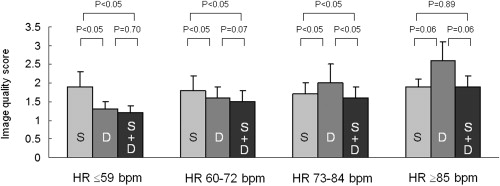
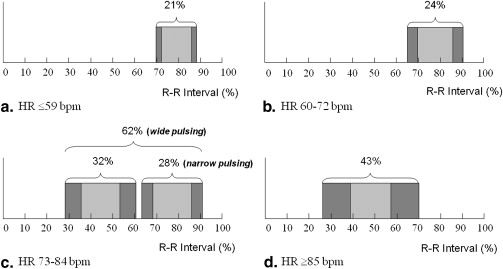
Table 3
Estimated Effective Dose of Retrospectively Gated CTCA without Tube Current Modulation and with the Proposed Model
HR ≤59 beats/min HR 60–73 beats/min HR 74–84 beats/min HR ≥85 beats/min Optimal pulsing windows ∗ (mean ± 2 standard deviation %) D 77.7 ± 3.6 D 77.8 ± 4.4 S 45.1 ± 6.8 D 77.1 ± 5.2 S 49.4 ± 12.2 With tube current modulation 20% tube current (mSv) † 5.3 5.3 8.7/8.9 § 6.6 0% tube current (mSv) ‡ 3.0 3.3 7.7/7.9 ‡ 5.2 No tube current modulation (mSv) 14.6 13.6 12.8 12.2
D, diastolic phase; HR, heart rate; S, indicates systolic.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Herzog B.A., Wyss C.A., Husmann L., et. al.: First head-to-head comparison of effective radiation dose from low-dose 64-slice CT with prospective ECG-triggering versus invasive coronary angiography. Heart 2009; 95: pp. 1656-1661.
2. Ehara M., Kawai M., Surmely J.F., et. al.: Diagnostic accuracy of coronary in-stent restenosis using 64-slice computed tomography: comparison with invasive coronary angiography. J Am Coll Cardiol 2007; 49: pp. 960-962.
3. Herzka D.A., Gharib A.M.: Should all patients with suspected coronary artery disease undergo coronary angiography with 16-row MDCT?. Nat Clin Pract Cardiovasc Med 2007; 4: pp. 74-75.
4. Motoyama S., Anno H., Sarai M., et. al.: Noninvasive coronary angiography with a prototype 256-row area detector computed tomography system comparison with conventional invasive coronary angiography. J Am Coll Cardiol 2008; 51: pp. 773-775.
5. Hausleiter J., Meyer T., Hermann F., et. al.: Estimated radiation dose associated with cardiac CT angiography. JAMA 2009; 301: pp. 500-507.
6. McCollough C.H., Primak A.N., Braun N., et. al.: Strategies for reducing radiation dose in CT. Radiol Clin North Am 2009; 47: pp. 27-40.
7. Hausleiter J., Meyer T., Hadamitzky M., et. al.: Radiation dose estimates from cardiac multislice computed tomography in daily practice: impact of different scanning protocols on effective dose estimates. Circulation 2006; 113: pp. 1305-1310.
8. Scheffel H., Alkadhi H., Leschka S., et. al.: Low-dose CT coronary angiography in the step-and-shoot mode: diagnostic performance. Heart 2008; 94: pp. 1132-1137.
9. Klass O., Walker M., Siebach A., et. al.: Prospectively gated axial CT coronary angiography: comparison of image quality and effective radiation dose between 64-and 256-slice CT. Eur Radiol 2010; 20: pp. 1124-1131.
10. Jakobs T.F., Becker C.R., Ohnesorge B., et. al.: Multislice helical CT of the heart with retrospective ECG gating: reduction of radiation exposure by ECG-controlled tube current modulation. Eur Radiol 2002; 12: pp. 1081-1086.
11. Weustink A.C., Mollet N.R., Pugliese F., et. al.: Optimal electrocardiographic pulsing windows and heart rate: effect on image quality and radiation exposure at dual-source coronary CT angiography. Radiology 2008; 248: pp. 792-798.
12. Law W.Y., Yang C.C., Chen L.K., et. al.: Retrospective gating vs. prospective triggering for noninvasive coronary angiography: assessment of image quality and radiation dose using a 256-slice CT scanner with 270 ms gantry rotation. Acad Radiol 2011; 18: pp. 31-39.
13. Cademartiri F., Nieman K., Lugt A., et. al.: Intravenous contrast material administration at 16-detector row helical CT coronary angiography: test bolus versus bolus-tracking technique. Radiology 2004; 233: pp. 817-823.
14. Austen W.G., Edwards J.E., Frye R.L., et. al.: A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 1975; 51: pp. 5-40.
15. International Commission on Radiological Protection: 2007 Recommendations of the International Commission on Radiological Protection (ICRP Publication 102). Ann ICRP 2007; 37: pp. 1-80.
16. Weigold W.G., Olszewski M.E., Walker M.J.: Low-dose prospectively gated 256-slice coronary computed tomographic angiography. Int J Cardiovasc Imaging 2009; 25: pp. 217-230.
17. Mok S.P.M., Yang C.C., Chen L.K., et. al.: Optimal systolic and diastolic image reconstruction windows for coronary 256-slice CT angiography. Acad Radiol 2010; 17: pp. 1386-1393.
18. Ohnesorge B.M., Flohr ThG, Becker C.R., et. al.: Multi-slice and dual-source CT in cardiac imaging.2nd ed.2007.Springer-VerlagHeidelberg, Berlin
19. Johnson T.R., Nikolaou K., Wintersperger B.J., et. al.: Dual-source CT cardiac imaging: initial experience. Eur Radiol 2006; 16: pp. 1409-1415.
20. Leschka S., Husmann L., Desbiolles L.M., et. al.: Optimal image reconstruction intervals for non-invasive coronary angiography with 64-slice CT. Eur Radiol 2006; 16: pp. 1964-1972.
21. Bley T.A., Ghanem N.A., Foell D., et. al.: Computed tomography coronary angiography with 370-milli-second gantry rotation time: evaluation of the best image reconstruction interval. J Comput Assist Tomogr 2005; 29: pp. 1-5.
22. Hamoir X.L., Flohr T., Hamoir V., et. al.: Coronary arteries: assessment of image quality and optimal reconstruction window in retrospective ECG-gated multislice CT at 375-ms gantry rotation time. Eur Radiol 2005; 15: pp. 296-304.
23. Chung C.S., Karamanoglu M., Kovács S.J.: Duration of diastole and its phases as a function of heart rate during supine bicycle exercise. Am J Physiol Heart Circ Physiol 2004; 287: pp. H2003-H2008.
24. Adler G., Meille L., Rohnean A., et. al.: Robustness of end-systolic reconstructions in coronary dual-source CT angiography for high heart rate patients. Eur Radiol 2010; 20: pp. 1118-1123.
25. Efstathopoulos E.P., Kelekis N.L., Pantos I., et. al.: Reduction of the estimated radiation dose and associated patient risk with prospective ECG-gated 256-slice CT coronary angiography. Phys Med Biol 2009; 54: pp. 5209-5222.