
Rationale and Objectives
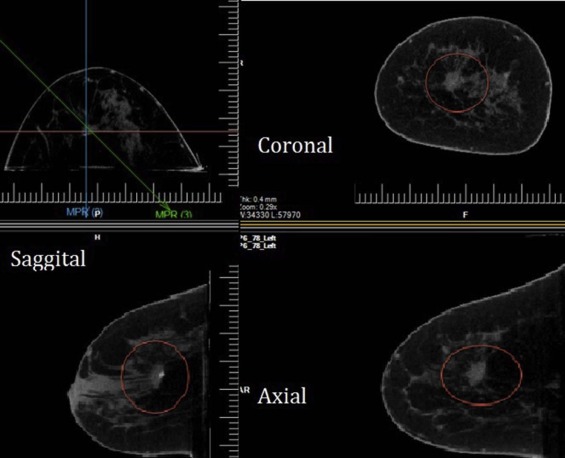
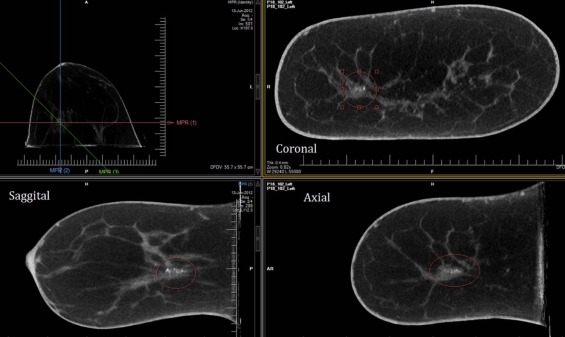
Dedicated breast computed tomography (DBCT) is an emerging and promising modality for breast lesions. The objective of this study was to evaluate the potential use of applying the BI-RADS Mammography Atlas 5th Edition for reporting and assessing breast lesions on DBCT. Currently, no atlas exists for DBCT.
Materials and Methods
Four radiologists trained in breast imaging were recruited in this institutional review board-approved, Health Insurance Portability and Accountability Act-compliant study. The enrolled radiologists, who were blinded to mammographic and histopathologic findings, individually reviewed 30 randomized DBCT cases that contained marked lesions. Thirty-four lesions were included in this study: 24 (70.6%) masses, 7 (20.6%) calcifications, and 3 (8.8%) architectural distortions. Eight (23.5%) lesions were malignant and 26 (76.5%) were benign. The reader was asked to specify according to the BI-RADS Mammography Atlas for each marked DBCT lesion: primary findings, features, breast density, and final assessment. We calculated readers’ diagnostic performances for differentiating between benign and malignant lesions and interobserver variability for reporting and assessing lesions using a generalized estimating equation and the Fleiss kappa (κ) statistic.
Results
The estimated overall sensitivity of the readers was 0.969, and the specificity was 0.529. There were no significant differences in the sensitivity and the specificity between lesion types. For reporting the presence of a primary finding, the overall substantial agreement (κ = 0.70) was seen. In assigning the breast density and the final assessment, the overall agreement was moderate (κ = 0.53) and fair (κ = 0.30).
Conclusion
The use of the BI-RADS Mammography Atlas 5th Edition for DBCT showed high performance and good agreement among readers.
Introduction
Breast Imaging Reporting and Data System (BI-RADS), established by the American College of Radiology, was begun in the late 1980s to address a lack of standardization and uniformity in mammography practice and reporting , and the BI-RADS lexicon has provided a valuable and reliable guide for reporting breast lesions on mammography, ultrasound, and magnetic resonance imaging (MRI), and has been familiar to most radiologists specializing in breast imaging. The descriptors in the BI-RADS lexicon have been selected on the basis of their ability to discriminate between benignity and malignancy as clear and standardized terms . BI-RADS has also recommended that a final impression be summarized by choosing only one among several standardized final assessment categories at the end of a report, each of which included a matched, standardized management recommendation . The BI-RADS atlas is intended to be a “living” document that changes as new data are acquired and more sophisticated patterns of breast care emerge . With continued evolvement of lesion characterization and assessment for malignancy, the BI-RADS Mammography Atlas is now in its fifth edition .
In addition to the updates in mammography, the fifth edition contains standardized breast lesion lexicons and assessment language for breast ultrasound and MRI. With advancements in breast imaging technologies, such as dedicated computed tomography of the breast, the BI-RADS Mammography Atlas can serve as the standard terminology upon which lexicons in other areas of radiology and research can be modeled.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Readers
Get Radiology Tree app to read full this article<
Data Description
Get Radiology Tree app to read full this article<
TABLE 1
Cross-Tabulation of Lesion Type and Pathology
Type Mass Calcification AD Total Pathology Benign, n (%) 19 (56) 5 (15) 2 (6) 26 (76) Malignant, n (%) 5 (15) 2 (6) 1 (3) 8 (24) Total, N (%) 24 (71) 7 (21) 3 (9) 34 (100)
AD, architectural distortion.
Get Radiology Tree app to read full this article<
Image Interpretation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 2
BI-RADS Atlas 5th Edition
Description Characteristic Masses Shape Oval Round Irregular Margin Circumscribed Obscured Microlobulated Indistinct Spiculated Density High density Equal density Low density Fat-containing Calcifications Typically benign Skin Vascular Coarse or “popcorn-like” Large rodlike Round Dystrophic Milk of calcium Suture Suspicious morphology Amorphous Coarse heterogenous Fine pleomorphic Fine linear or fine-linear branching Distribution Diffuse Regional Grouped Linear Segmental Architectural distortion Yes No Asymmetry Asymmetry Global asymmetry Focal asymmetry Developing asymmetry
Get Radiology Tree app to read full this article<
Data Analysis and Statistics
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Performances
Get Radiology Tree app to read full this article<
TABLE 3
Sensitivities and Specificities of Readers for Different Lesion Types
Mass and AD Calcification Overall Sensitivity Specificity Sensitivity Specificity Sensitivity Specificity Reader 1 1.000 0.762 1.000 0.200 1.000 0.654 Reader 2 1.000 0.762 1.000 0.600 1.000 0.731 Reader 3 0.833 0.476 1.000 0.400 0.875 0.462 Reader 4 1.000 0.286 1.000 0.200 1.000 0.269
AD, architectural distortion.
Get Radiology Tree app to read full this article<
Interobserver Variability
Get Radiology Tree app to read full this article<
TABLE 4
Interobserver Variability in Description of Mammographic Lesions
BI-RADS Descriptor Kappa Value Presence of primary finding Overall 0.70 Mass and architectural distortion 0.78 Calcification 0.52 Breast density Overall 0.53 Final assessment Overall 0.30 Mass and architectural distortion 0.22 Calcification 0.56
BI-RADS, Breast Imaging Reporting and Data System.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. McLelland R., Hendrick R., Zinninger M.D., et. al.: The American College of Radiology mammography accreditation program. AJR Am J Roentgenol 1991; 157: pp. 473-479.
2. Getty D.J., Pickett R.M., D’Orsi C.J., et. al.: Enhanced interpretation of diagnostic images. Invest Radiol 1988; 23: pp. 240-252.
3. Swets J.A., Getty D.J., Pickett R.M., et. al.: Enhancing and evaluating diagnostic accuracy. Med Decis Making 1991; 11: pp. 9-17.
4. Burnside E.S., Sickles E.A., Bassett L.W., et. al.: The ACR BI-RADS® experience: learning from history. J Am Coll Radiol 2009; 6: pp. 851-860.
5. Committee ACoRB-R , Radiology ACo : Breast Imaging Reporting and Data System.1998.American College of RadiologyReston, VA
6. D’Orsi C.J.: ACR BI-RADS Atlas: Breast Imaging Reporting and Data System.2013.American College of RadiologyReston, VA
7. Coburn N.G., Chung M.A., Fulton J., et. al.: Decreased breast cancer tumor size, stage, and mortality in Rhode Island: an example of a well-screened population. Cancer Control 2004; 11: pp. 222-230.
8. Jatoi I., Chen B.E., Anderson W.F., et. al.: Breast cancer mortality trends in the United States according to estrogen receptor status and age at diagnosis. J Clin Oncol 2007; 25: pp. 1683-1690.
9. Otto S., Fracheboud J., Looman C., et. al.: National evaluation team for breast cancer screening initiation of population-based mammography screening in Dutch municipalities and effect on breast-cancer mortality: a systematic review. Lancet 2003; 361: pp. 411-417.
10. Gordon P.B., Goldenberg S.L.: Malignant breast masses detected only by ultrasound. A retrospective review. Cancer 1995; 76: pp. 626-630.
11. Pisano E.D., Gatsonis C., Hendrick E., et. al.: Diagnostic performance of digital versus film mammography for breast-cancer screening. NEJM 2005; 353: pp. 1773-1783.
12. Bach A.G., Abbas J., Jasaabuu C., et. al.: Comparison between incidental malignant and benign breast lesions detected by computed tomography: a systematic review. J Med Imaging Radiat Oncol 2013; 57: pp. 529-533.
13. Boone J.M., Nelson T.R., Lindfors K.K., et. al.: Dedicated breast CT: radiation dose and image quality evaluation 1. Radiology 2001; 221: pp. 657-667.
14. Chang C., Sibala J.L., Fritz S.L., et. al.: Computed tomographic evaluation of the breast. Am J Roentgenol 1978; 131: pp. 459-464.
15. Chang C.J., Sibala J.L., Gallagher J.H., et. al.: Computed tomography of the breast: a preliminary report 1. Radiology 1977; 124: pp. 827-829.
16. Chen B., Ning R.: Cone-beam volume CT breast imaging: feasibility study. Med Phys 2002; 29: pp. 755-770.
17. Gisvold J., Karsell P., Reese E.: Clinical evaluation of computerized tomographic mammography. Mayo Clin Proc 1977; pp. 181-185.
18. Gong X., Vedula A.A., Glick S.J.: Microcalcification detection using cone-beam CT mammography with a flat-panel imager. Phys Med Biol 2004; 49: pp. 2183.
19. Inoue K., Liu F., Hoppin J., et. al.: High-resolution computed tomography of single breast cancer microcalcifications in vivo. Mol Imaging 2012; 11: pp. 1.
20. Kuzmiak C.M., Cole E.B., Zeng D., et. al.: Dedicated three-dimensional breast computed tomography: lesion characteristic perception by radiologists. J Clin Imaging Sci 2016; 6:
21. Kwan A.L., Boone J.M., Yang K., et. al.: Evaluation of the spatial resolution characteristics of a cone-beam breast CT scanner. Med Phys 2007; 34: pp. 275-281.
22. Lai C.-J., Shaw C.C., Chen L., et. al.: Visibility of microcalcification in cone beam breast CT: effects of x-ray tube voltage and radiation dose. Med Phys 2007; 34: pp. 2995-3004.
23. Lindfors K.K., Boone J.M., Nelson T.R., et. al.: Dedicated breast CT: initial clinical experience 1. Radiology 2008; 246: pp. 725-733.
24. McKinley R.L., Tornai M.P., Tuttle L.A., et. al.: Development and initial demonstration of a low-dose dedicated fully 3D breast CT system. International Workshop on Digital Mammography.2012.SpringerHeidelberg, Germanypp. 442-449.
25. Mettivier G., Russo P., Lanconelli N., et. al.: Cone-beam breast computed tomography with a displaced flat panel detector array. Med Phys 2012; 39: pp. 2805-2819.
26. O’Connell A., Conover D.L., Zhang Y., et. al.: Cone-beam CT for breast imaging: radiation dose, breast coverage, and image quality. Am J Roentgenol 2010; 195: pp. 496-509.
27. O’Connell A.M., Karellas A., Vedantham S.: The potential role of dedicated 3D breast CT as a diagnostic tool: review and early clinical examples. Breast J 2014; 20: pp. 592-605.
28. O’Connell A.M., Kawakyu-O’Connor D.: Dedicated cone-beam breast computed tomography and diagnostic mammography: comparison of radiation dose, patient comfort, and qualitative review of imaging findings in BI-RADS 4 and 5 lesions. J Clin Imaging Sci 2012; 2: pp. 7.
29. Prionas N.D., Lindfors K.K., Ray S., et. al.: Contrast-enhanced dedicated breast CT: initial clinical experience 1. Radiology 2010; 256: pp. 714-723.
30. Shen Y., Zhong Y., Lai C.-J., et. al.: Cone beam breast CT with a high pitch (75 µm), thick (500 µm) scintillator CMOS flat panel detector: visibility of simulated microcalcifications. Med Phys 2013; 40: pp. 101915.
31. Zhao B., Zhang X., Cai W., et. al.: Cone beam breast CT with multiplanar and three dimensional visualization in differentiating breast masses compared with mammography. Eur J Radiol 2015; 84: pp. 48-53.
32. Aminololama-Shakeri S., Abbey C.K., Gazi P., et. al.: Differentiation of ductal carcinoma in-situ from benign micro-calcifications by dedicated breast computed tomography. Eur J Radiol 2016; 85: pp. 297-303.
33. Lazarus E., Mainiero M.B., Schepps B., et. al.: BI-RADS lexicon for US and mammography: interobserver variability and positive predictive value. Radiology 2006; 239: pp. 385-391.