
Rationale and Objectives
Magnetic resonance imaging (MRI) characteristics of Breast Imaging Reporting and Data System (BI-RADS) 4 and 5 lesions were evaluated to identify characteristics that may improve the positive predictive value (PPV) of a biopsy.
Materials and Methods
MRI BI-RADS 4 or 5 breast findings in 101 women who underwent biopsy leading to a diagnosis of cancer within 1 year (PPV 3 ; n = 115 cases) were reviewed. Patient history, lesion morphology, enhancement pattern and kinetics, and T 2 characteristics were examined.
Results
The PPV 3 of all BI-RADS 4 and 5 breast lesions seen on MRI was 22.6% (26 of 115). Excluding lesions with second-look imaging correlates decreased the PPV 3 to 11.8% (6/51). Of the MRI-guided biopsies, 20.9% (24 of 115) yielded a high-risk lesion, altering surgical management. MRI lesion type did not significantly affect the PPV 3 : the PPV 3 was 26.3% (15 of 57) for masses, 21.4% (9 of 42) for non mass enhancement (NME) and 12.5% (2 of 16) for suspicious foci. The PPV 3 for lesions found on diagnostic MRI in women with newly diagnosed cancer was 30.8% (20 of 65) which was statistically significantly greater compared to a PPV 3 of 11.9% (5 of 42) for lesions identified on high-risk screening MRI.
Conclusions
Suspicious MRI findings identified on a second-look examination are more likely malignant than those seen only on MRI. Suspicious MRI findings discovered in patients with concurrent malignancy have a greater PPV 3 than those detected on high-risk screening MRIs. However, the type of MRI finding (mass vs. NME vs. foci) does not significantly affect the PPV 3 and should not be used as a discriminator for determining biopsy threshold.
Breast magnetic resonance imaging (MRI) is a highly sensitive imaging tool in the detection and characterization of breast cancer . MRI is useful in the evaluation of women with a new diagnosis of breast cancer to determine the extent of disease and screen the contralateral breast when there is a new diagnosis . There is also evidence that supplemental screening with MRI when women have a lifetime chance of malignancy of 20% is beneficial . Breast MRI is highly sensitive but less specific than ultrasound (US) or mammography . As a result, the recommendation for biopsy of a suspicious lesion may yield cancer in a lesser percentage of patients than when mammograms or US are used to diagnose cancer. Therefore, suspicious MRI findings would be expected to have a decreased positive predictive value (PPV 3 ) when compared to the PPV for suspicious findings identified on mammography and US.
There are a number of MRI characteristics that are considered predictive of malignancy, such as Breast Imaging Reporting and Data System (BI-RADS) assessment , lesion size , enhancement pattern , and enhancement kinetics . However, there is considerable overlap between suspicious and benign MRI characteristics.
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Method of Biopsy of Suspicious MRI Findings
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Histologic Outcome of Suspicious MRI Findings
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Characteristics of Suspicious MRI Findings
Get Radiology Tree app to read full this article<
Table 1
Characteristics of Biopsy-Proven Malignancies
Characteristic Number of Carcinomas Invasive or In Situ Invasive In Situ Lesion type Mass 15 11 4 NME 9 5 4 Foci 2 2 0 Pattern of enhancement Homogeneous 15 11 4 Heterogeneous 10 6 4 Peripheral 1 1 0 Early enhancement kinetics Rapid 13 9 4 Medium 11 8 3 Slow 2 1 1 Late enhancement kinetics Persistent 5 3 2 Plateau 10 7 3 Washout 11 8 3 T 1 Hyperintense 0 0 0 Hypointense 13 10 3 Isointense 13 8 5 T 2 Hyperintense 16 11 5 Hypointense 1 1 0 Isointense 7 5 2 Slightly hyperintense 2 1 1 Total 26 18 8
Get Radiology Tree app to read full this article<
Morphology
Get Radiology Tree app to read full this article<
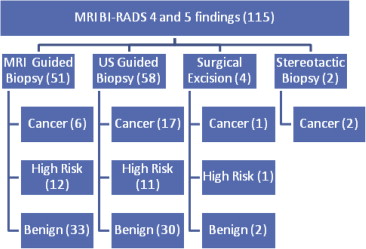
![Figure 3, Imaging characteristics of suspicious MRI findings: Suspicious MRI findings according to MRI morphologic type (mass, NME, or focus) with subsequent method of biopsy and pathologic results. High risk refers to the histologic classification of the lesion (ie, lobular neoplasia, atypical ductal hyperplasia [ADH], radial scar, papillary lesion). BI-RADS, Breast Imaging Reporting and Data System; MRI, magnetic resonance imaging.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/PPV3ofSuspiciousBreastMRIFindings/2_1s20S1076633214002761.jpg)
Get Radiology Tree app to read full this article<
Masses
Get Radiology Tree app to read full this article<
Non Mass Enhancement
Get Radiology Tree app to read full this article<
Foci
Get Radiology Tree app to read full this article<
Pattern of Enhancement
Get Radiology Tree app to read full this article<
Enhancement Kinetics
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
T 2 Characteristics
Get Radiology Tree app to read full this article<
Indication for Breast MRIs
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Suspicious MRI Findings That Did Not Enhance on Day of Biopsy
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Method of Biopsy of Suspicious MRI Findings
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Characteristics of Suspicious MRI Findings
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Morphology
Get Radiology Tree app to read full this article<
Pattern of Enhancement
Get Radiology Tree app to read full this article<
Enhancement Kinetics
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
T 2 Characteristics
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Indication for Breast MRIs
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Strengths of the Study
Get Radiology Tree app to read full this article<
Limitations of the Study
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Lehman C.D., Blume J.D., Weatherall P., et. al.: Screening women at high risk for breast cancer with mammography and magnetic resonance imaging. Cancer 2005; 103: pp. 1898-1905.
2. Lehman C.D., Schnall M.D.: Imaging in breast cancer: magnetic resonance imaging. Breast Cancer Research 2005; 7: pp. 215.
3. Lehman C.D., Schnall M.D., Kuhl C.K., et. al.: Report of the Working Groups on Breast MRI: Report of the High-Risk Screening Group. The Breast Journal 2004; 10: pp. S9-S12.
4. Liberman L., Mason G., Morris E.A., et. al.: Does size matter? Positive predictive value of MRI-detected breast lesions as a function of lesion size. American Journal of Roentgenology 2006; 186: pp. 426-430.
5. DeMartini W.B., Lehman C.D., Peacock S., et. al.: Computer-aided detection applied to breast MRI: assessment of CAD-generated enhancement and tumor sizes in breast cancers before and after neoadjuvant chemotherapy 1 . Academic Radiology 2005; 12: pp. 806-814.
6. Harms S., Flamig D., Hesley K., et. al.: MR imaging of the breast with rotating delivery of excitation off resonance: clinical experience with pathologic correlation. Radiology 1993; 187: pp. 493-501.
7. Lehman C.D., Blume J.D., Thickman D., et. al.: Added cancer yield of MRI in screening the contralateral breast of women recently diagnosed with breast cancer: results from the International Breast Magnetic Resonance Consortium (IBMC) trial. Journal of Surgical Oncology 2005; 92: pp. 9-15.
8. Schnall M.D., Blume J., Bluemke D.A., et. al.: MRI detection of distinct incidental cancer in women with primary breast cancer studied in IBMC 6883. Journal of Surgical Oncology 2005; 92: pp. 32-38.
9. Lehman C.D., Gatsonis C., Kuhl C.K., et. al.: MRI evaluation of the contralateral breast in women with recently diagnosed breast cancer. New England Journal of Medicine 2007; 356: pp. 1295-1303.
10. Lee S.G., Orel S.G., Woo I.J., et. al.: MR imaging screening of the contralateral breast in patients with newly diagnosed breast cancer: preliminary results. Radiology 2003; 226: pp. 773-778.
11. Liberman L., Morris E.A., Dershaw D.D., et. al.: MR imaging of the ipsilateral breast in women with percutaneously proven breast cancer. American Journal of Roentgenology 2003; 180: pp. 901-910.
12. Institute NC. Available at: https://irep.nci.nih.gov/radrat .
13. Lee C.H., Dershaw D.D., Kopans D., et. al.: Breast cancer screening with imaging: recommendations from the Society of Breast Imaging and the ACR on the use of mammography, breast MRI, breast ultrasound, and other technologies for the detection of clinically occult breast cancer. Journal of the American College of Radiology 2010; 7: pp. 18-27.
14. Sardanelli F., Podo F., D’Agnolo G., et. al.: Multicenter comparative multimodality surveillance of women at genetic-familial high risk for breast cancer (HIBCRIT study): interim results. Radiology 2007; 242: pp. 698-715.
15. Leach M.O., Boggis C., Dixon A., et. al.: Screening with magnetic resonance imaging and mammography of a UK population at high familial risk of breast cancer: a prospective multicentre cohort study (MARIBS). Lancet 2005; 365: pp. 1769-1778.
16. Warner E., Plewes D.B., Hill K.A., et. al.: Surveillance of BRCA1 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA 2004; 292: pp. 1317-1325.
17. Kriege M., Brekelmans C.T., Boetes C., et. al.: Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. New England Journal of Medicine 2004; 351: pp. 427-437.
18. Causer P.A., Jong R.A., Warner E., et. al.: Breast cancers detected with imaging screening in the BRCA population: emphasis on MR imaging with histopathologic correlation. Radiographics 2007; 27: pp. S165-S182.
19. Kuhl C.K., Schmutzler R.K., Leutner C.C., et. al.: Breast MR imaging screening in 192 women proved or suspected to be carriers of a breast cancer susceptibility gene: preliminary results. Radiology 2000; 215: pp. 267-279.
20. Lehman C.D., Isaacs C., Schnall M.D., et. al.: Cancer yield of mammography, MR, and US in high-risk women: prospective multi-institution breast cancer screening study. Radiology 2007; 244: pp. 381-388.
21. Kuhl C.: The current status of breast MR imaging part I. Choice of technique, image interpretation, diagnostic accuracy, and transfer to clinical practice. Radiology 2007; 244: pp. 356-378.
22. Goscin C.P., Berman C.G., Clark R.A.: Magnetic resonance imaging of the breast. Cancer control 2001; 8: pp. 399-406.
23. Peters N.H., Rinkes I.H.B., Zuithoff N.P., et. al.: Meta-Analysis of MR imaging in the diagnosis of breast lesions. Radiology 2008; 246: pp. 116-124.
24. Mahoney M.C., Gatsonis C., Hanna L., et. al.: Positive predictive value of BI-RADS MR imaging. Radiology 2012; 264: pp. 51-58.
25. Langer S.A., Horst K.C., Ikeda D.M., et. al.: Pathologic correlates of false positive breast magnetic resonance imaging findings: which lesions warrant biopsy?. The American Journal of Surgery 2005; 190: pp. 633-640.
26. Sakamoto N., Tozaki M., Higa K., et. al.: Categorization of non-mass-like breast lesions detected by MRI. Breast Cancer 2008; 15: pp. 241-246.
27. Liberman L., Morris E.A., Dershaw D.D., et. al.: Ductal enhancement on MR imaging of the breast. American Journal of Roentgenology 2003; 181: pp. 519-525.
28. Kuhl C.K., Mielcareck P., Klaschik S., et. al.: Dynamic breast MR imaging: are signal intensity time course data useful for differential diagnosis of enhancing lesions?. Radiology 1999; 211: pp. 101-110.
29. Macura K.J., Ouwerkerk R., Jacobs M.A., et. al.: Patterns of enhancement on breast MR images: interpretation and imaging pitfalls. Radiographics 2006; 26: pp. 1719-1734. quiz
30. Kuhl C.K., Bieling H.B., Gieseke J., et. al.: Healthy premenopausal breast parenchyma in dynamic contrast-enhanced MR imaging of the breast: normal contrast medium enhancement and cyclical-phase dependency. Radiology 1997; 203: pp. 137-144.
31. Müller-Schimpfle M., Ohmenhaüser K., Stoll P., et. al.: Menstrual cycle and age: influence on parenchymal contrast medium enhancement in MR imaging of the breast. Radiology 1997; 203: pp. 145-149.
32. Delille J.P., Slanetz P.J., Yeh E.D., et. al.: Physiologic changes in breast magnetic resonance imaging during the menstrual cycle: perfusion imaging, signal enhancement, and influence of the T1 relaxation time of breast tissue. The breast journal 2005; 11: pp. 236-241.
33. (ACR) ACoR. Breast Imaging Reporting and Data System Atlas (BI-RADS® Atlas). 4th ed ed. Reston, Virginia 2003.
34. Naeger D.M., Kohi M.P., Webb E.M., et. al.: Correctly using sensitivity, specificity, and predictive values in clinical practice: how to avoid three common pitfalls. American Journal of Roentgenology 2013; 200: pp. W566-W570.
35. Yamaguchi K., Schacht D., Sennett C.A., et. al.: Decision making for breast lesions initially detected at contrast-enhanced breast MRI. American Journal of Roentgenology 2013; 201: pp. 1376-1385.
36. Han B.-K., Schnall M.D., Orel S.G., et. al.: Outcome of MRI-guided breast biopsy. American Journal of Roentgenology 2008; 191: pp. 1798-1804.
37. Arazi-Kleinman T., Skair-Levy M., Slonimsky E., et. al.: JOURNAL CLUB: is screening MRI indicated for women with a personal history of breast cancer? Analysis based on biopsy results. American Journal of Roentgenology 2013; 201: pp. 919-927.
38. Morris E.A., Liberman L., Ballon D.J., et. al.: MRI of occult breast carcinoma in a high-risk population. American Journal of Roentgenology 2003; 181: pp. 619-626.
39. Warner E., Messersmith H., Causer P., et. al.: Systematic review: using magnetic resonance imaging to screen women at high risk for breast cancer. Annals of Internal Medicine 2008; 148: pp. 671-679.
40. Bassett L.W., Hendrick R.E.: Quality determinants of mammography: clinical practice guideline.2004.DIANE Publishing
41. Linda A., Zuiani C., Londero V., et. al.: Outcome of initially only magnetic resonance mammography-detected findings with and without correlate at second-look sonography: distribution according to patient history of breast cancer and lesion size. The Breast 2008; 17: pp. 51-57.
42. DeMartini W.B., Eby P.R., Peacock S., et. al.: Utility of targeted sonography for breast lesions that were suspicious on MRI. American Journal of Roentgenology 2009; 192: pp. 1128-1134.
43. Abe H., Schmidt R.A., Shah R.N., et. al.: MR-directed (“Second-Look”) ultrasound examination for breast lesions detected initially on MRI: MR and sonographic findings. American Journal of Roentgenology 2010; 194: pp. 370-377.
44. Baltzer P.A., Benndorf M., Dietzel M., et. al.: False-positive findings at contrast-enhanced breast MRI: a BI-RADS descriptor study. American Journal of Roentgenology 2010; 194: pp. 1658-1663.
45. Liberman L., Morris E.A., Lee M.J.-Y., et. al.: Breast lesions detected on MR imaging: features and positive predictive value. American Journal of Roentgenology 2002; 179: pp. 171-178.
46. Orel S., Mendonca M.H., Reynolds C., et. al.: MR imaging of ductal carcinoma in situ. Radiology 1997; 202: pp. 413-420.
47. Facius M., Renz D.M., Neubauer H., et. al.: Characteristics of ductal carcinoma in situ in magnetic resonance imaging. Clinical Imaging 2007; 31: pp. 394-400.
48. Gutierrez R.L., DeMartini W.B., Eby P.R., et. al.: BI-RADS lesion characteristics predict likelihood of malignancy in breast MRI for masses but not for nonmasslike enhancement. American Journal of Roentgenology 2009; 193: pp. 994-1000.
49. Wedegärtner U., Bick U., Wörtler K., et. al.: Differentiation between benign and malignant findings on MR-mammography: usefulness of morphological criteria. European Radiology 2001; 11: pp. 1645-1650.
50. Kuhl C.K., Klaschik S., Mielcarek P., et. al.: Do T2-weighted pulse sequences help with the differential diagnosis of enhancing lesions in dynamic breast MRI?. Journal of Magnetic Resonance Imaging : JMRI 1999; 9: pp. 187-196.
51. Malich A., Fischer D.R., Wurdinger S., et. al.: Potential MRI interpretation model: differentiation of benign from malignant breast masses. American Journal of Roentgenology 2005; 185: pp. 964-970.
52. Bartella L., Liberman L., Morris E.A., et. al.: Nonpalpable mammographically occult invasive breast cancers detected by MRI. American Journal of Roentgenology 2006; 186: pp. 865-870.
53. Gutierrez R.L., DeMartini W.B., Eby P., et. al.: Clinical indication and patient age predict likelihood of malignancy in suspicious breast MRI lesions. Academic Radiology 2009; 16: pp. 1281-1285.
54. Bosmans H., Marshall N.: Radiation doses and risks associated with mammographic screening. Current Radiology Reports 2013; 1: pp. 30-38.
55. Wiratkapun C., Duke D., Nordmann A.S., et. al.: Indeterminate or suspicious breast lesions detected initially with MR imaging: value of MRI-directed breast ultrasound. Academic Radiology 2008; 15: pp. 618-625.
56. Hylton N. American College of Radiology Imaging Network ACRIN 6698 Diffusion weighted MR imaging biomarkers for assessment of breast cancer response to neoadjuvant treatment: a sub-study of the I-SPY 2 TRIAL (Investigation of Serial Studies to Predict Your Therapeutic Response with Imaging and Molecular Analysis).