
Rationale and Objectives
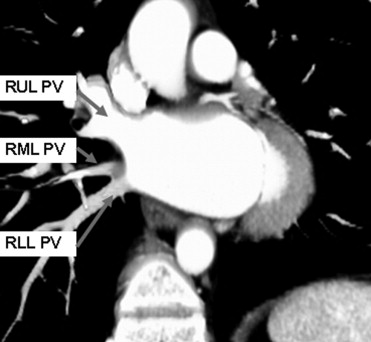
Evaluate the role of two-dimensional echocardiography and electrocardiographically (ECG)-gated contrast-enhanced multislice computed tomographic (MSCT) cardiac imaging to assess cardiac anatomy, specifically pulmonary venous anatomy and left atrial thrombus, in a selected group of patients before catheter-based atrial fibrillation ablation.
Materials and Methods
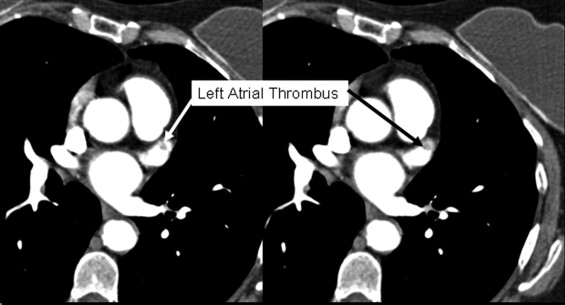
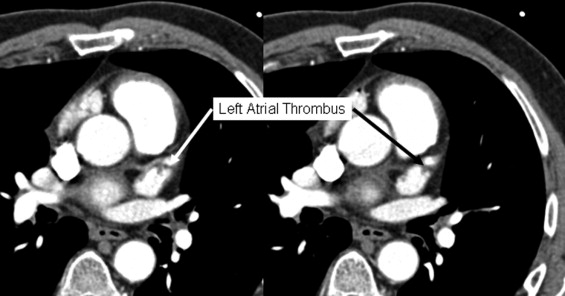
Left atrial anatomy and associated findings in 34 consecutive patients scheduled for electrophysiologic testing who underwent both echocardiography and ECG-gated 16-slice MSCT cardiac imaging were retrospectively compared. Results from two-dimensional transthoracic echocardiography (TTE), cardiac MSCT, electrophysiologic study (EPS), and transesophageal echocardiography (TEE) (when performed) were taken from the official medical record without prior knowledge of this study when interpretation was rendered for clinical use. Electronic record review included: presence of left atrial thrombus (defined as constant filling defect on at least two echocardiographic views or filling defect on computed tomography) and location, pulmonary venous anatomy, and other cardiac, mediastinal, or pulmonary abnormalities.
Results
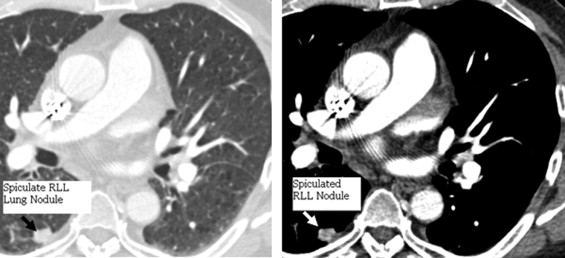
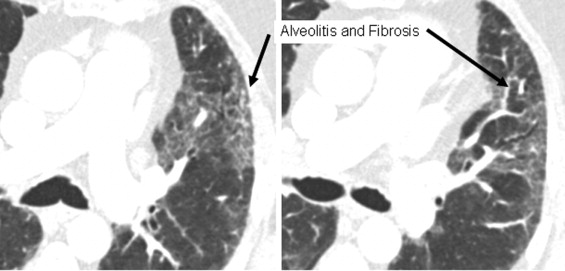
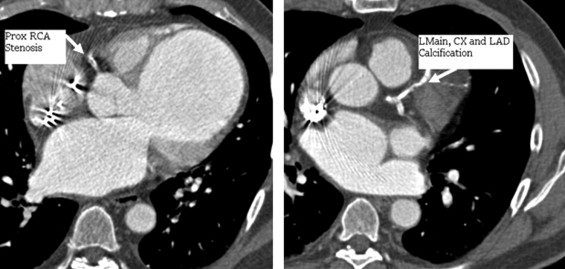
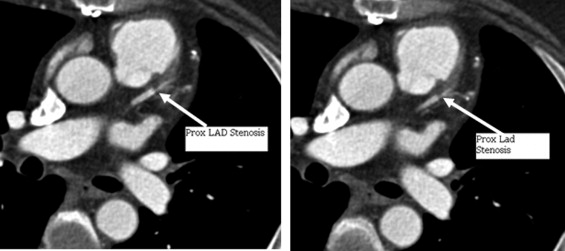
Left atrial thrombus was identified by cardiac MSCT alone in five patients (15%). Pulmonary venous variants were identified with cardiac MSCT in two patients (6%). Both MSCT and echocardiography were normal in 17 subjects (79%). Echocardiography was better at identifying associated valvular abnormalities that were seen in 10 patients (29%). Cardiac MSCT angiography alone identified other cardiac and noncardiac abnormalities, including suspicious pulmonary malignancy, mediastinal adenopathy, and coronary stenosis in 15 patients (44%).
Conclusions
Echocardiography and cardiac MSCT angiography often provide complimentary findings during the preprocedural evaluation for patients with atrial fibrillation requiring ablation. Cardiac MSCT may provide significant additional information about the left atrium, mediastinum, coronary circulation, and visualized lung fields. Based on this study, we would advise that patients considered for radiofrequency ablation for uncontrolled right atrial fibrillation have both echocardiography and ECG-gated contrast-enhanced cardiac MSCT performed as part of the preprocedure evaluation.
Patients with atrial fibrillation nonresponsive to medical treatment are increasingly referred for electrophysiologic testing (EPS) for catheter ablation. Many of these patients are at increased risk of left atrial thrombus, even with adequate anticoagulation, putting them at risk for systemic embolism syndromes (particularly with manipulation in the left atrium). Left atrial thrombus has been evaluated by transthoracic echocardiography (TTE), transesophageal echocardiography (TEE), and electron beam ultrafast (cine) computed tomography (UFCCT) of the heart ( ). The availability of TTE, anatomic detail of the cardiac chambers, and minimal side effects made TTE evaluation of the heart commonplace. However, a recent study comparing TTE with UFCCT suggested that UFCCT was better at detecting intracardiac masses and thrombus in the left atrial appendage ( ). In another study in patients with mitral valve disease or myocardial infarction, UFCCT was also deemed superior both to TTE and cardiac angiography ( ). Focus was then shifted from TTE to TEE for the detection of left atrial thrombus.
Many recent articles have substantiated the better detection of left atrial thrombus, particularly in the left atrial appendage by TEE compared to TTE ( ). A majority of these authors recommend TEE if normal findings are found on TTE during investigation of the left atrium when assessing cardiac origins of distal emboli. Variables on TTE with strong negative predictive value for findings of left atrial thrombus during subsequent TEE have been defined, and these may limit the use of TEE, albeit that TEE remains the reference method ( ).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Comparison of Results with Cardiac MSCT Angiography and Echocardiography for Total Agreement in All Left Atrial Findings (a) and Agreement Concerning Presence of Left Atrial Thrombus Only (b)
TTE (a) Detection of All Left Atrial Abnormalities Evaluation Number of Patients (%) MSCT (−) TTE (−) 27/34 (79%) MSCT (+) TTE (−) 7/34 (21%) MSCT (−) TTE (+) 0/0 (0%) MSCT (+) TTE (+) 0/0 (0%) (b) Detection of Left Atrial Thrombus MSCT (−) TTE (−) 29/34 (85%) MSCT (+) TEE (−) 5/34 (15%) MSCT (−) TTE (+) 0/0 (0%) MSCT (+) TTE (+) 0/0 (0%)
TEE (a) Detection of All Left Atrial Abnormalities Evaluation Number of Patients (%) MSCT (−) TTE (−) 9/16 (56%) MSCT (+) TTE (−)7/16 (44%) MSCT (−) TTE (+) 0/0 (0%) MSCT (+) TTE (+) 0/0 (0%) (b) Detection of Left Atrial Thrombus Evaluation Number of Patients (%) MSCT (−) TTE (−) 12/16 (75%) MSCT (+) TTE (−)4/16 (25%) MSCT (−) TTE (+) 0/0 (0%) MSCT (+) TTE (+) 0/0 (0%)
MSCT, cardiac multislice computed tomography; TEE, transesophageal echocardiography; +, abnormality detected; −, no abnormality detected (normal).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Cardiac and Noncardiac Findings by MSCT Not Visualized by TEE
Cardiac findings Number of Patients Left atrial thrombus 5 Anomalous pulmonary veins 2 Noncardiac findings Number of Patients Occult, suspicious lung nodules 3 Coronary artery disease 4 Pulmonary edema 1 Pulmonary fibrosis 1
MSCT, cardiac multislice computed tomography; TEE, transesophageal echocardiography.

Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Love B.B., Struck L.K., Stanford W., et. al.: Comparison of two-dimensional echocardiography and ultrafast cardiac computed tomography for evaluating intracardiac thrombi in cerebral ischemia. Stroke 1990; 21: pp. 1033-1038.
2. Tomoda H., Hoshiai M., Furuya H., et. al.: Evaluation of intracardiac thrombus with computed tomography. Am J Cardiol 1983; 51: pp. 843-852.
3. Kitayama H., Kiuchi K., Endo T., et. al.: Value of cardiac ultrafast computed tomography for detecting right atrial thrombi in chronic atrial fibrillation. Am J Cardiol 1997; 79: pp. 1292-1295.
4. Helgason C.M., Chomka E., Louie E., et. al.: The potential role for ultrafast cardiac computed tomography in patients with stroke. Stroke 1989; 20: pp. 465-472.
5. Bleiweis M.S., Georgiou D., Brundage B.H.: Detection of intracardiac masses by ultrafast computed tomography. Am J Cardiol 1994; 8: pp. 63-68.
6. Nakanishi T., Hamada S., Takamiya M., et. al.: A pitfall in ultrafast CT scanning for the detection of left atrial thrombi. J Comput Assist Tomogr 1993; 17: pp. 42-45.
7. Masuda Y., Morooka N., Yoshida H., et. al.: Noninvasive diagnosis of thrombus in the heart and large vessels-usefulness of two-dimensional echocardiography and X-ray CT. Jap Circ 1984; 48: pp. 83-89.
8. Rousso I., Deviri E., Lerner M.A., et. al.: CT diagnosis of left atrial thrombus undiagnosed by echocardiography. Comp Radiol 1984; 8: pp. 293-296.
9. Jaber W.A., Prior D.L., Thamilarasan M., et. al.: Efficacy of anticoagulation in resolving left atrial and left atrial appendage thrombi a transesophageal echocardiographic study. Am Heart J 2000; 140: pp. 150-156.
10. Agmon Y., Khandhria B.K., Gentile F., et. al.: Echocardiographic assessment of the left atrial appendage. J Am Coll Cardiol 1999; 34: pp. 1867-1877.
11. Saady N.M., Obel O.A., Camm A.J.: Left atrial appendage structure, function and role in thromboembolism. Heart 1999; 82: pp. 547-555.
12. Carerj M.P., Trifiro A., Granata F., et. al.: Comparison between transesophageal echocardiography and transthoracic echocardiography with harmonic tissue imaging for left atrial appendage assessment. Clin Cardiol 2002; 25: pp. 268-270.
13. Omran H., Jung W., Rabahieh P., et. al.: Imaging of thrombi and assessment of left atrial appendage function a prospective study comparing transthoracic and transesophageal echocardiography. Heart 1999; 81: pp. 192-198.
14. deBruijn S.F., Agema W.R., Lammers G.J., et. al.: Transesophageal echocardiography is superior to transthoracic echocardiography in management of patients of any age with transient ischemic attack or stroke. Stroke 2006; 37: pp. 2531-2534.
15. Khan G.N., Dairywala I.T., Liu Z., et. al.: Three-dimensional echocardiography of left atrial appendage thrombus. Echocardiography 2001; 18: pp. 163-166.
16. Arrigo F., Carerj S., Pizzimenti G.: Role of transesophageal echocardiography in the study of embolism of cardiac origin. Cardiologia 1993; 38: pp. 301-317.
17. Hwang J.J., Chen J.J., Lin S.C., et. al.: Diagnostic accuracy of transesophageal echocardiography for detecting left atrial thrombi in patients with rheumatic heart disease having undergone mitral valve operations. Am J Cardiol 1993; 72: pp. 677-681.
18. Ellis K., Ziada K.M., Vivekananthan D., et. al.: Transthoracic echocardiographic predictors of left atrial appendage thrombus. Am J Cardiol 2006; 97: pp. 421-425.
19. Toyoda K., Yasak M., Nagata S., et. al.: Transesophageal echocardiography for detecting intracardiac thrombi in embolic stroke. Angiology 1993; 44: pp. 376-383.
20. Uchiyama S., Yamazaki M., Iwata M., et. al.: Diagnosis of intracardiac thrombi by various imaging techniques and activation of platelets and coagulation-fibrinolysis in patients with cardioembolic stroke. Rinsho Shinkeigaku 1996; 36: pp. 429-435.
21. Tani T., Yamakami S., Okamoto M., et. al.: Usefulness of electron beam tomography in the prone position for detecting atrial thrombi in chronic atrial fibrillation. J Comput Assist Tomogr 2003; 27: pp. 78-84.
22. Nakanishi T., Hamada S., Takamiya M., et. al.: A pitfall in ultrafast CT scanning for the detection of left atrial thrombi. J Comput Assist Tomogr 1993; 17: pp. 42-45.
23. Alam G., Addo F., Malik M., et. al.: Detection of left atrial appendage thrombus by spiral CT scan. Echocardiography 2003; 20: pp. 99-100.
24. DeLange S.: Limitations of transesophageal ultrasound in the assessment of intracardiac masses: a case report. Rev Esp Anestesiol Reanim 2005; 52: pp. 421-424.
25. Jaber W.A., White R.D., Luzmiak S.A., et. al.: Comparison of ability to identify left atrial thrombus by three-dimensional tomography versus transesophageal echocardiography in patients with atrial fibrillation. Am J Cardiol 2004; 4: pp. 486-489.
26. Maksimovic R., Filippo C., Scholten M., et. al.: Sixteen-row multislice computed tomography in the assessment of pulmonary veins prior to ablative treatment: validation vs conventional pulmonary venography and study of reproducibility. Eur Radiol 2004; 14: pp. 369-374.
27. Shapiro M, Dodd JD, Brad TJ, et al. Common pulmonary venous ostium of the right and left inferior pulmonary veins: an unusual pulmonary vein anomaly depicted with 64-slice cardiac computed tomography. J Cardiovasc Electrophysiol 200; 18:110.
28. Lawler L.P., Fishman E.K.: Thoracic venous anatomy multidetector row CT evaluation. Radiol Clin North Am 2003; 41: pp. 545-560.
29. Gupta H., Mayo-Smith W.W., Mainiero M.B., et. al.: Helical CT of pulmonary vascular abnormalities. AJR Am J Roentgenol 2002; 178: pp. 478-492.
30. Piorkowski C., Hindricks G., Schreiber , et. al.: Eletroanatomic reconstruction of the left atrium, pulmonary veins, and esophagus compared with the “true anatomy” on multislice computed tomography in patients undergoing catheter ablation of atrial fibrillation. Heart Rhythm 2006; 3: pp. 317-327.
31. Wongcharoen W., Tsao H.M., Wu M.H., et. al.: Preexisting pulmonary vein stenosis in patients undergoing atrial fibrillation ablation: a report of five cases. J Cardiovasc Electrophysiol 2006; 17: pp. 423-425.
32. Maksimovic R., Scholten M.F., Cademartire F., et. al.: Sixteen multidetector row computed tomography of pulmonary veins: 3-months’ follow-up after treatment of paroxysmal atrial fibrillation with cryothermal ablation. Eur Radiol 2005; 15: pp. 1122-1127.
33. Burgstahler C., Trabold T., Kuettner A., et. al.: Visualization of pulmonary vein stenosis after radiofrequency ablation using multi-slice computed tomography: initial clinical experience in 33 patients. Int J Cardiol 2005; 102: pp. 2. 287–291
34. Trabold T., Kuttner A., Keuschmid M., et. al.: Visualization of pulmonary vein stenosis after radio-frequency ablation for treatment of atrial fibrillation using multidetector computed tomography with retrospective gating. Rofo Fortschr Geg Rontgenstr Neuen Bildgeb Verfahr 2003; 175: pp. 89-93.
35. Maksimovic R., Dill T., Ristic A.D., et. al.: Imaging in Percutaneous ablation for atrial fibrillation. Eur Radiol 2006; 16: pp. 249-504.
36. Saad E.B., Marrouche F.N., Saad C.P., et. al.: Pulmonary vein stenosis after catheter ablation of atrial fibrillation: emergence of a new clinical syndrome. Ann Intern Med 2003; 138: pp. 634-638.