
Rationale and Objectives
Lung resection for primary bronchogenic carcinoma in the setting of chronic obstructive pulmonary disease often requires a detailed assessment of lung function to avoid perioperative complications and long-term disability. The aim of this study was to test the hypothesis that a novel technique of spiral computed tomographic (CT) subtraction imaging provides accuracy equal to the current standard of radioisotope perfusion scintigraphy in predicting postoperative lung function.
Methods and Materials
Preoperative lung function, radioisotope perfusion scintigraphy, spiral CT subtraction imaging, and assessment of postoperative lung function were performed in 25 patients with surgically resectable primary bronchogenic carcinoma. Comparisons of predicted postoperative lung function between the two modalities and to true postoperative lung function were performed using Pearson’s correlation and linear regression analysis.
Results
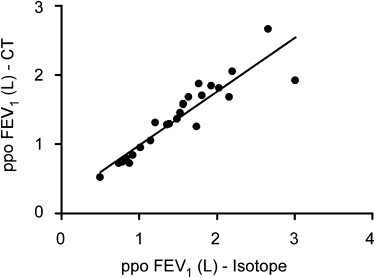
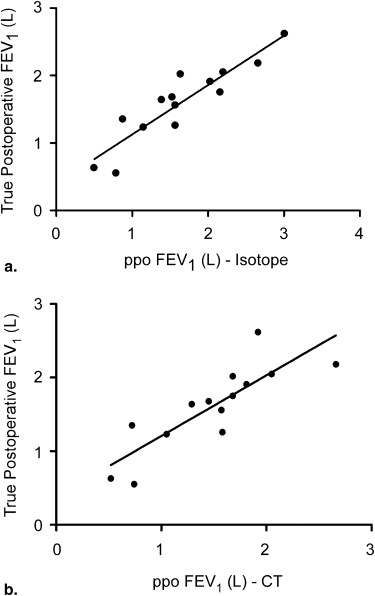
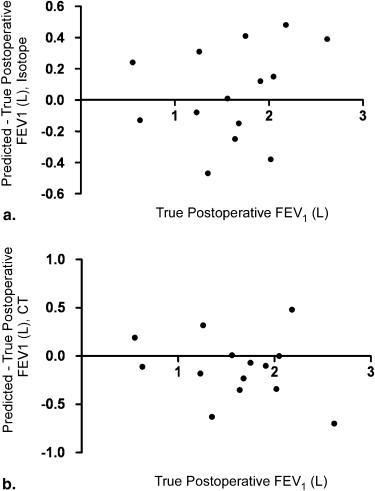
Among the 25 patients enrolled in the study, there was a high degree of agreement between the predicted value of postoperative forced expiratory lung volume in 1 second (FEV 1 ) generated on novel contrast CT subtraction imaging and that on radioisotope perfusion scintigraphy ( r = 0.96, P < .001). Furthermore, there was a strong correlation between the predicted and actual postoperative FEV 1 values for both imaging modalities ( r = 0.87, P < .001, and r = 0.88, P < .001, respectively), among the 14 patients completing the study protocol.
Conclusion
A novel technique of CT subtraction imaging is equally accurate at predicting postoperative lung function as radioisotope perfusion scintigraphy, which may obviate the need for additional nuclear imaging in the context of the preoperative assessment of resectable lung cancer in high-risk patients.
Primary bronchogenic carcinoma remains the leading cause of cancer death in both men and women worldwide . Despite advances in chemotherapy and radiation therapy, surgical resection continues to offer the best long-term survival for patients with localized non-small-cell lung cancer . Unfortunately, many of these patients also have chronic airflow limitations related to cigarette smoking, a factor that has been associated with an increased risk for perioperative complications and long-term disability following lung resection . As a result, a detailed physiologic assessment, including efforts to predict postoperative lung function, has become an integral component of the preoperative assessment for these patients.
Presently, the investigation most commonly used for the prediction of postoperative pulmonary function following lung resection surgery is quantitative radioisotope perfusion scintigraphy. Using perfusion as a surrogate for ventilation, this method enables the determination of relative contribution of the region of lung to be resected to the overall ventilatory function. Perfusion scintigraphy has been shown to be relatively accurate in predicting postoperatively the spirometric forced expiratory lung volume in 1 second (FEV 1 ) following resectional surgery, with correlation coefficients between predicted and true postoperative FEV 1 being variably reported from 0.81 to 0.92 . This demonstrated accuracy, combined with both the availability and noninvasive nature of this test, has led to its inclusion in the guidelines of the European Respiratory Society and the American College of Chest Physicians for patients with non-small-cell lung cancer and impaired lung function being evaluated for lung resection .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Methods and materials
Patient Selection
Get Radiology Tree app to read full this article<
Study Design
Get Radiology Tree app to read full this article<
Spirometry
Get Radiology Tree app to read full this article<
Radioisotope Perfusion Scintigraphy
Get Radiology Tree app to read full this article<
Contrast CT Subtraction Imaging
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Surgical Procedures
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Patients
Get Radiology Tree app to read full this article<
Table 1
Summary of Patient Demographics, Operations, and FEV 1 Data
PPO FEV 1 (L) Patient Age (y) Sex Preoperative FEV 1 (L) Surgical Procedure Radioisotope Perfusion Scintigraphy CT Imaging True Postoperative FEV 1 (L) 1 61 M 2.75 Lobectomy 2.20 2.05 2.05 2 56 F 0.68 Lobectomy 0.50 0.52 0.63 3 67 M 1.92 Bilobectomy 1.39 1.29 1.64 4 58 F 2.06 Pneumonectomy 1.15 1.05 1.23 5 73 M 2.00 Lobectomy 1.57 1.58 1.26 6 61 M 2.03 Lobectomy 1.77 1.87 Died 7 82 M 1.55 Lobectomy 1.49 1.36 Unresectable 8 52 M 1.96 Lobectomy 1.57 1.57 1.56 9 69 M 1.50 Pneumonectomy 1.02 0.95 Unresectable 10 75 F 1.48 Lobectomy 1.36 1.28 Died 11 66 M 0.98 Lobectomy 0.74 0.72 Unresectable 12 56 F 2.30 Lobectomy 2.16 1.68 1.75 13 51 F 2.95 Lobectomy 2.66 2.66 2.18 14 76 M 1.60 Pneumonectomy 0.88 0.72 1.35 15 55 F 2.10 Lobectomy 1.93 1.84 Died 16 71 M 1.86 Lobectomy 1.53 1.45 1.68 17 54 F 1.35 Lobectomy 1.21 1.31 Unresectable 18 73 F 0.92 Lobectomy 0.79 0.74 0.55 19 71 M 3.31 Pneumonectomy 3.01 1.92 2.62 20 75 M 1.98 Lobectomy 1.74 1.25 Unresectable 21 67 M 0.98 Lobectomy 0.92 0.84 Unresectable 22 52 F 2.21 Lobectomy 1.64 1.68 2.02 23 76 M 2.23 Lobectomy 2.03 1.81 1.91 24 54 M 2.71 Pneumonectomy 1.81 1.70 Unresectable 25 78 F 0.99 Lobectomy 0.84 0.79 Unresectable
CT, computed tomographic; FEV1, forced expiratory volume in 1 second.
Get Radiology Tree app to read full this article<
Surgical Procedures and Outcomes
Get Radiology Tree app to read full this article<
Agreement Between Imaging Modalities
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Accuracy of Predicting Postoperative Lung Function
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Jemal A., Murray T., Ward E., et. al.: Cancer statistics, 2005. CA Cancer J Clin 2005; 55: pp. 10-30.
2. Win T., Jackson A., Sharples L., et. al.: Relationship between pulmonary function and lung cancer surgical outcome. Eur Respir J 2005; 25: pp. 594-599.
3. Reif M., Socinski M., Rivera M.: Evidence-based medicine in the treatment of non-small-cell lung cancer. Clin Chest Med 2000; 21: pp. 107-120.
4. Datta D., Lahiri B.: Preoperative evaluation of patients undergoing lung resection surgery. Chest 2003; 123: pp. 2096-2103.
5. Corris P., Ellis D., Hawkins T., et. al.: Use of radionuclide scanning in the preoperative estimation of pulmonary function after pneumonectomy. Thorax 1987; 42: pp. 285-291.
6. Colice G., Shafazand S., Griffin J., et. al.: Physiologic evaluation of the patient with lung cancer being considered for resectional surgery. Chest 2007; 132: pp. 161S-177S.
7. Brunelli A., Charloux A., Bolliger C.T., et. al.: ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur Respir J 2009; 34: pp. 16-41.
8. Markos J., Mullan B., Hillman D., et. al.: Preoperative assessment as a predictor of mortality and morbidity after lung resection. Am Rev Respir Dis 1989; 139: pp. 902-910.
9. Bolliger C., Wyser C., Roser H., et. al.: Lung scanning and exercise testing for the prediction of postoperative performance in lung resection candidates at increased risk for complications. Chest 1995; 108: pp. 341-348.
10. Bolliger C., Guckel C., Engel H., et. al.: Prediction of functional reserves after lung resection: comparison between quantitative computed tomography, scintigraphy, and anatomy. Respiration 2002; 69: pp. 482-489.
11. Pate P., Tenholder M., Griffin J., et. al.: Preoperative assessment of the high-risk patient for lung resection. Ann Thorac Surg 1996; 61: pp. 1494-1500.
12. Brunelli A., Refai M., Monteverde M., et. al.: Predictors of early morbidity after major lung resection in patients with and without airflow limitation. Ann Thorac Surg 2002; 74: pp. 999-1003.
13. Uramoto H., Nakanishi R., Fujino Y., et. al.: Prediction of pulmonary complications after a lobectomy in patients with non-small cell lung cancer. Thorax 2001; 56: pp. 59-61.
14. Iizasa T., Suzuki M., Yasufuku K., et. al.: Preoperative pulmonary function as a prognostic factor for stage I non-small cell lung carcinoma. Ann Thorac Surg 2004; 77: pp. 1896-1903.
15. Wang J.: Pulmonary function tests in preoperative pulmonary evaluation. Respir Med 2004; 98: pp. 598-605.
16. Brunelli A., Fianchini A.: Predicted postoperative FEV1 and complications in lung resection candidates. Chest 1997; 111: pp. 1145.
17. Pierce R., Copland J., Sharpe K., et. al.: Preoperative risk evaluation for lung cancer resection: predicted postoperative product as a predictor of surgical mortality. Am J Respir Crit Care Med 1994; 150: pp. 947-955.
18. Kearney D., Lee T., Reilly J., et. al.: Assessment of operative risk in patients undergoing lung resection. Importance of predicted pulmonary function. Chest 1994; 105: pp. 753-759.
19. Mitsudomi T., Mizoue T., Yoshimatsu T., et. al.: Postoperative complications after pneumonectomy for treatment of lung cancer: multivariate analysis. J Surg Oncol 1996; 61: pp. 218-222.
20. Silvestri G., Gould M., Margolis M., et. al.: Noninvasive staging of non-small cell lung cancer. Chest 2007; 132: pp. 178S-201S.
21. Kristersson S., Lindell S., Strandberg L.: Prediction of pulmonary function loss due to pneumonectomy using 133Xe-radioisometry. Chest 1972; 62: pp. 696-698.
22. American Thoracic Society: Standardization of spirometry: 1994 update. Am J Respir Crit Care Med 1995; 152: pp. 1107-1136.
23. Bland J., Altman D.: Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: pp. 307-310.
24. Wu M., Chang J., Chiang A., et. al.: Use of quantitative CT to predict postoperative lung function in patients with lung cancer. Radiology 1994; 191: pp. 257-262.
25. Wu W., Pan H., Chiang A., et. al.: Prediction of postoperative lung function in patients with lung cancer: comparison of quantitative CT with perfusion scintigraphy. AJR Am J Roentgenol 2002; 178: pp. 667-672.
26. Wernly J., De Meester T., Kirchner P., et. al.: Clinical value of quantitative ventilation perfusion lung scans in the surgical management of bronchogenic carcinoma. Chest 1980; 80: pp. 535-547.
27. Thibault J.B., Sauer K.D., Bouman C.A., et. al.: A three-dimensional statistical approach to improved image quality for multislice helical CT. Med Phys 2007; 34: pp. 4526-4544.