
Rationale and Objectives
The objective of this study was to investigate predictors of pain associated with computed tomographic arthrography of the shoulder.
Materials and Methods
Before shoulder arthrography, all participants were assessed with the Hospital Anxiety and Depression Scale (HADS) and the World Health Organization Quality of Life Short Version Instrument (WHOQOL-BREF). The participants were nonrandomized into two groups: the anesthesia group, who underwent prior local infiltration anesthesia before shoulder arthrography, and the nonanesthesia group, who did not undergo prior local infiltration anesthesia. The pain levels at intraprocedure, at 1, 2, 6, and 12 hours, and at 1 and 2 days after injection were assessed by using a visual analog scale. Univariate and multivariate generalized linear model analyses were conducted.
Results
Sixty participants in the anesthesia group and 60 participants in the nonanesthesia group were included. The pain level at intraprocedure (3.37 ± 1.94 in the anesthesia group and 3.20 ± 1.34 in the nonanesthesia group) was the highest of the whole pain course. The psychological domain ( P = .0013) of WHOQOL-BREF, gender ( P = .042), body mass index ( P = .0001), and the total number of reinsertion and redirection of needle ( P < .0001) were independent predictors of arthrography-related pain.
Conclusions
The pain associated with shoulder computed tomographic arthrography depends on the psychological domain of WHOQOL-BREF, gender, body mass index, and the total number of reinsertion and redirection of needle.
Introduction
Computed tomographic arthrography (CTA) is a well-established imaging method for evaluating shoulder disorders and normal variants , which include rotator cuff tears, capsulolabral complex lesions and variants, osseous and cartilage lesions, and postoperative pathology. Since the early 2000s, commercialized multidetector computed tomography with a capacity to acquire a large imaging volume of isotropic submillimeter voxels within a short scan time, which could be reformatted in multiplane with high spatial resolution, has substantially improved the diagnostic performance of CTA and broadened its applications in the musculoskeletal system . Shoulder arthrography is an invasive procedure in which contrast media is injected into the joint via a needle. Side effects of this procedure, especially for arthrography-related pain and discomfort, have often been reported . The pain is rated mild or fairly severe, which usually lasts for several days. According to a biopsychosocial model, perception of pain is not only correlated with biological factors but also affected by social and psychological factors . The complete predictors of pain associated with CTA, including social and psychological factors, are of interest for radiologists and referring physicians to educate patients. During a shoulder geometry study using the CTA technique , we designed a concomitant prospective study to investigate predictors of pain associated with CTA of the shoulder.
Materials and Methods
Participants
This prospective nonrandomized study was approved and supervised by the institutional review board (IRB) with written informed consent from every participant. As part of a previously IRB-approved study at our institution, 134 volunteers were recruited to undergo CTA of the shoulder to study proximal humerus anatomy. Each volunteer was paid $75 for participation. An additional study was appended to the existing IRB approval to examine the predictors of pain associated with shoulder CTA. To evaluate the potential influence of local infiltration anesthesia during shoulder arthrography, participants were assigned into either the anesthesia group or the nonanesthesia group. Participants were excluded from the study if they had bone or soft tissue abnormalities on CTA; withdrew from an ongoing study; had taken analgesics such as acetaminophen or NSAIDs to relieve postarthrographic pain; had unsuccessful arthrography; were unavailable for a telephone interview; or were uncooperative to fill out anxiety, depression, and quality of life questionnaires.
Hospital Anxiety and Depression Scale (HADS)
Get Radiology Tree app to read full this article<
World Health Organization Quality of Life Short Version Instrument (WHOQOL-BREF)
Get Radiology Tree app to read full this article<
Arthrography Procedure
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Computed Tomography (CT)
Get Radiology Tree app to read full this article<
Pain Assessment
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Participants
Get Radiology Tree app to read full this article<
TABLE 1
Summary of Participant-related and Procedure-related Predictors Between the Anesthesia and the Nonanesthesia Groups
Factor Anesthesia Group Nonanesthesia Group_P_ Participant-related factors Age .85 <25 23 (38.3) 24 (40) ≥25 37 (61.7) 36 (60) Gender .71 Male 32 (53.33) 34 (56.67) Female 28 (46.67) 26 (43.33) BMI 22.02 ± 2.83 22.10 ± 3.13 .88 Anxiety .57 Yes 8 (13.33) 6 (10) No 52 (86.67) 54 (90) Depression 1.00 Yes 5 (8.33) 5 (8.33) No 55 (91.67) 55 (91.67) WHOQOL-BREF Physical health 72.38 ± 13.36 71.07 ± 11.42 .57 Psychological 68.54 ± 12.55 68.61 ± 11.85 .98 Social relationships 69.44 ± 13.87 65.56 ± 12.79 .11 Environment 60.36 ± 17.92 57.86 ± 14.84 .41 Procedure-related factors Contrast volume 4.55 ± 2.01 4.06 ± 1.30 .11 TNRRN 1.53 ± 1.66 1.25 ± 1.67 .35 Side .80 Left 50 (83.33) 51 (85) Right 10 (16.67) 9 (15)
BMI, body mass index; TNRRN, total number of reinsertion and redirection of needle; WHOQOL-BREF, World Health Organization Quality of Life Short Version Instrument.
Data are mean ± standard deviations or number of participants, with percentages in parentheses.
Get Radiology Tree app to read full this article<
Pain Levels Assessment
Get Radiology Tree app to read full this article<
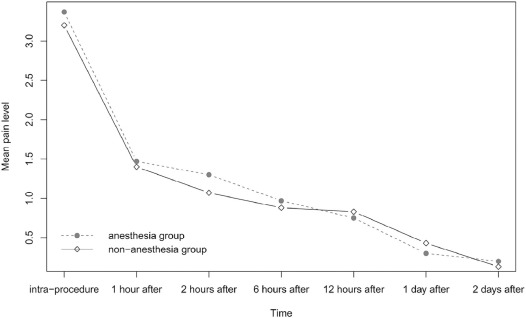
TABLE 2
Comparison at Different Time Points Between the Anesthesia and the Nonanesthesia Groups and Multiple Comparisons
Time Point Anesthesia Group Nonanesthesia Group_P_ \* Intraprocedure 3.37 a 3.2 a .59 1 h after injection 1.47 b 1.4 b .73 2 h after injection 1.3 b 1.07 c .21 6 h after injection 0.97 b,c 0.88 c .66 12 h after injection 0.75 c 0.83 c .65 1 d after injection 0.3 d 0.43 d .31 2 d after injection 0.2 d 0.13 d .44
Means followed by the same letter in a column do not differ significantly (alpha = 0.05) according to Student-Newman-Keuls analysis.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Significance of Results
Get Radiology Tree app to read full this article<
TABLE 3
Univariate and Multivariate Analyses to Identify the Independent Predictors of Arthrography-related Pain
Variable Univariate Analysis Multivariate Analysis Coefficient 95% CI_P_ Coefficient 95% CI_P_ Age ≥25 0.20 (−0.08 to 0.49) .1577 Gender (female) 0.39 (0.11–0.66) .0059 0.3491 (0.01–0.69) .042 BMI 0.06 (0.01–0.11) .0132 0.1105 (0.05–0.17) .0001 Anxiety −0.44 (−0.89 to 0.01) .0529 −0.3346 (−0.83 to 0.16) .1882 Depression −0.09 (−0.58 to 0.41) .7268 WHOQOL-BREF Physical health 0.001 (−0.01 to 0.01) .8711 Psychological −0.02 (−0.03 to −0.01) .0009 −0.0267 (−0.04 to −0.01) .0013 Social relationships 0.01 (−0.004 to 0.02) .2154 Environment −0.01 (−0.02 to 0.0006) .0677 −0.0048 (−0.02 to 0.01) .4275 Contrast volume 0.01 (−0.07 to 0.09) .7949 TNRRN 0.28 (0.20–0.36) <.0001 0.2649 (0.17–0.36) <.0001 Side −0.09 (−0.46 to 0.29) .6427 LIA −0.11 (−0.38 to 0.17) .4421 −0.2176 (−0.52 to 0.09) .1588
BMI, body mass index; CI, confidence interval; LIA, local infiltration anesthesia; TNRRN, total number of reinsertion and redirection of needle; WHOQOL-BREF, World Health Organization Quality of Life Short Version Instrument.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Charousset C., Bellaiche L., Duranthon L.D., et. al.: Accuracy of CT arthrography in the assessment of tears of the rotator cuff. J Bone Joint Surg Br 2005; 87: pp. 824-828.
2. Cochet H., Couderc S., Pele E., et. al.: Rotator cuff tears: should abduction and external rotation (ABER) positioning be performed before image acquisition? A CT arthrography study. Eur Radiol 2010; 20: pp. 1234-1241.
3. De Filippo M., Bertellini A., Sverzellati N., et. al.: Multidetector computed tomography arthrography of the shoulder: diagnostic accuracy and indications. Acta Radiol 2008; 49: pp. 540-549.
4. Fritz J., Fishman E.K., Small K.M., et. al.: MDCT arthrography of the shoulder with datasets of isotropic resolution: indications, technique, and applications. AJR Am J Roentgenol 2012; 198: pp. 635-646.
5. Kim Y.J., Choi J.A., Oh J.H., et. al.: Superior labral anteroposterior tears: accuracy and interobserver reliability of multidetector CT arthrography for diagnosis. Radiology 2011; 260: pp. 207-215.
6. Lecouvet F.E., Simoni P., Koutaissoff S., et. al.: Multidetector spiral CT arthrography of the shoulder. Clinical applications and limits, with MR arthrography and arthroscopic correlations. Eur J Radiol 2008; 68: pp. 120-136.
7. Nourissat G., Tribot-Laspiere Q., Aim F., et. al.: Contribution of MRI and CT arthrography to the diagnosis of intra-articular tendinopathy of the long head of the biceps. Orthop Traumatol Surg Res 2014; 100: pp. S391-S394.
8. Oh J.H., Kim J.Y., Choi J.A., et. al.: Effectiveness of multidetector computed tomography arthrography for the diagnosis of shoulder pathology: comparison with magnetic resonance imaging with arthroscopic correlation. J Shoulder Elbow Surg 2010; 19: pp. 14-20.
9. Omoumi P., Bafort A.C., Dubuc J.E., et. al.: Evaluation of rotator cuff tendon tears: comparison of multidetector CT arthrography and 1.5-T MR arthrography. Radiology 2012; 264: pp. 812-822.
10. Omoumi P., Rubini A., Dubuc J.E., et. al.: Diagnostic performance of CT-arthrography and 1.5T MR-arthrography for the assessment of glenohumeral joint cartilage: a comparative study with arthroscopic correlation. Eur Radiol 2015; 25: pp. 961-969.
11. Rhee R.B., Chan K.K., Lieu J.G., et. al.: MR and CT arthrography of the shoulder. Semin Musculoskelet Radiol 2012; 16: pp. 3-14.
12. Nishii T., Tanaka H., Nakanishi K., et. al.: Fat-suppressed 3D spoiled gradient-echo MRI and MDCT arthrography of articular cartilage in patients with hip dysplasia. AJR Am J Roentgenol 2005; 185: pp. 379-385.
13. Waldt S., Bruegel M., Ganter K., et. al.: Comparison of multislice CT arthrography and MR arthrography for the detection of articular cartilage lesions of the elbow. Eur Radiol 2005; 15: pp. 784-791.
14. De Filippo M., Araoz P.A., Pogliacomi F., et. al.: Recurrent superior labral anterior-to-posterior tears after surgery: detection and grading with CT arthrography. Radiology 2009; 252: pp. 781-788.
15. Hall F.M., Rosenthal D.I., Goldberg R.P., et. al.: Morbidity from shoulder arthrography: etiology, incidence, and prevention. AJR Am J Roentgenol 1981; 136: pp. 59-62.
16. Giaconi J.C., Link T.M., Vail T.P., et. al.: Morbidity of direct MR arthrography. AJR Am J Roentgenol 2011; 196: pp. 868-874.
17. Saupe N., Zanetti M., Pfirrmann C.W., et. al.: Pain and other side effects after MR arthrography: prospective evaluation in 1085 patients. Radiology 2009; 250: pp. 830-838.
18. Binkert C.A., Zanetti M., Hodler J.: Patient’s assessment of discomfort during MR arthrography of the shoulder. Radiology 2001; 221: pp. 775-778.
19. Choo H.J., Lee S.J., Kim D.W., et. al.: Intraarticular local anesthesia: can it reduce pain related to MR or CT arthrography of the shoulder?. AJR Am J Roentgenol 2013; 200: pp. 860-867.
20. Vranceanu A.M., Barsky A., Ring D.: Psychosocial aspects of disabling musculoskeletal pain. J Bone Joint Surg Am 2009; 91: pp. 2014-2018.
21. Zhang Q., Shi L.L., Ravella K.C., et. al.: Distinct proximal humeral geometry in Chinese population and clinical relevance. J Bone Joint Surg Am 2016; 98: pp. 2071-2081.
22. Bjelland I., Dahl A.A., Haug T.T., et. al.: The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res 2002; 52: pp. 69-77.
23. The WHOQOL Group: Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med 1998; 28: pp. 551-558.
24. Steurer-Dober I., Rufibach K., Hodler J., et. al.: Do patients with structural abnormalities of the shoulder experience pain after MR arthrography of the shoulder?. Radiology 2010; 256: pp. 870-878.
25. Huskisson E.C.: Measurement of pain. Lancet 1974; 2: pp. 1127-1131.
26. Koivikko M.P., Koskinen S.K.: Is subcutaneous local anesthesia in shoulder magnetic resonance arthrography necessary?. Acta Radiol 2007; 48: pp. 741-743.
27. Spick C., Szolar D.H., Reittner P., et. al.: MR arthrography of the shoulder: do we need local anesthesia?. Eur J Radiol 2014; 83: pp. 980-983.
28. Storey T.F., Gilbride G., Clifford K.: Postprocedural pain in shoulder arthrography: differences between using preservative-free normal saline and normal saline with benzyl alcohol as an intraarticular contrast diluent. AJR Am J Roentgenol 2014; 203: pp. 1059-1062.
29. Johansen J.G., Berner A.: Arthrography with Amipaque (metrizamide) and other contrast media. A roentgenographic and histologic evaluation in rabbits. Invest Radiol 1976; 11: pp. 534-540.
30. Hajek P.C., Sartoris D.J., Gylys-Morin V., et. al.: The effect of intra-articular gadolinium-DTPA on synovial membrane and cartilage. Invest Radiol 1990; 25: pp. 179-183.
31. Cooper D.E., O’Brien S.J., Warren R.F.: Supporting layers of the glenohumeral joint. An anatomic study. Clin Orthop Relat Res 1993; 289: pp. 144-155.
32. Blanchard T.K., Bearcroft P.W., Dixon A.K., et. al.: Magnetic resonance imaging or arthrography of the shoulder: which do patients prefer?. Br J Radiol 1997; 70: pp. 786-790.
33. McKendall M.J., Haier R.J.: Pain sensitivity and obesity. Psychiatry Res 1983; 8: pp. 119-125.