
Rationale and Objectives
To determine whether emergency department (ED) preliminary reports rendered by subspecialist attending radiologists who are reading outside their field of expertise are more accurate than reports rendered by radiology residents, and to compare error rates between radiologists and nonradiologists in the ED setting.
Materials and Methods
The study was performed at a large academic medical center with a busy ED. An electronic preliminary report generator was used in the ED to capture preliminary interpretations rendered in a clinical setting by radiology residents, junior attendings (within 2 years of taking their oral boards), senior attendings, and ED clinicians between August 1999 and November 2004. Each preliminary report was later reviewed by a final interpreting radiologist, and the preliminary interpretation was adjudicated for the presence of substantial discordances, defined as a difference in interpretation that might immediately impact the care of the patient. Of the 612,890 preliminary reports in the database, 65,780 (11%) met inclusion criteria for this study. A log-linear analysis was used to assess the effects of modality and type of author on preliminary report error rates.
Results
ED clinicians had significantly higher error rates when compared with any type of radiologist, regardless of modality. Within the radiologists, residents and junior attendings had lower error rates than did senior attendings, but the differences were not statistically significant.
Conclusion
Subspecialized attending radiologists who interpret ED examinations outside their area of expertise have error rates similar to those of radiology residents. Nonradiologists have significantly higher error rates than radiologists and radiology residents when interpreting examinations in the ED.
Academic radiology departments have traditionally allowed radiology residents to preliminarily interpret examinations performed in the emergency department (ED) after normal working hours, and provide a preliminary report to the referring clinicians. The following morning, these preliminary interpretations are subjected to scrutiny by subspecialist radiologists, who render final interpretations. In recent years, however, many academic departments have begun providing after-hours service from attending radiologists ( ). The continuous presence of attending radiologists is presumed to result in better patient care because fewer diagnostic errors will be made ( ).
In some radiology departments, there are dedicated, subspecialized emergency radiologists who cover both daytime and nighttime shifts in the ED. At other institutions, general radiologists (“nighthawks”) are hired to exclusively cover the night hours. In many departments, however, radiologists who are subspecialized in areas other than emergency radiology cover the ED in turn. These radiologists are often required to interpret examinations outside their field of subspecialization. It is unclear whether subspecialized attending radiologists, particularly those who have been subspecialized for many years, can provide a higher level of patient care than a radiology resident on call.
Get Radiology Tree app to read full this article<
Materials and methods
Setting
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
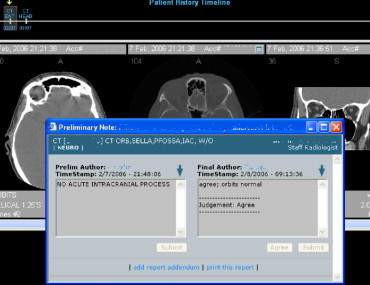
Preliminary Report Tool
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Adjudication
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Validation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Exclusion Criteria
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Rates of Substantial Discordance Between Preliminary and Final Interpretations of Emergency Department Radiology Examinations
Clinician Resident Senior Staff Junior Staff All Physicians CR 867/35536 (2.4%) 12/1499 (0.8%) 3/553 (0.5%) 3/374 (0.8%) 885/37962 (2.3%) CT 32/778 (4.1%) 333/16385 (2.0%) 88/3587 (2.5%) 98/5440 (1.8%) 551/26190 (2.1%) Other 0/24 (0%) 11/1293 (0.9%) 0/72 (0%) 2/239 (0.8%) 13/1628 (0.8%) All modalities 899/36338 (2.5%) 356/19177 (1.9%) 91/4212 (2.2%) 103/6053 (1.7%) 1449/65780 (2.2%)
CR: conventional radiograph; CT: computed tomography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Select Pairwise Comparisons of Error Rates for Preliminary Reports
Modality Author Type 1 vs. Author Type 2 95% CI Significant? CR Clinician (2.4%) Resident (0.8%) 1.2% to 2.1% Yes CT Clinician (4.1%) Senior staff (2.5%) 0.2% to 3.1% Yes CT Clinician (4.1%) Resident (2.0%) 0.6% to 3.5% Yes CR Resident (0.8%) Senior staff (0.5%) −0.5% to 1.0% No CT Senior staff (2.5%) Resident (2.0%) −0.1% to 1.0% No
Numbers in parentheses are error rates.
95% CI: 95% confidence interval for difference of percentages.
Statistical significance is defined as P < .05.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Hunter T.B., Krupinski E.A., Hunt K.R., et. al.: Emergency department coverage by academic departments of radiology. Acad Radiol 2000; 7: pp. 165-170.
2. Velmahos G.C., Fili C., Vassiliu P., et. al.: Around-the-clock attending radiology coverage is essential to avoid mistakes in the care of trauma patients. Am Surg 2001; 67: pp. 1175-1177.
3. Branstetter B.F.: Are residents’ on-call errors worse than the alternatives?. J Am Coll Radiol 2005; 2: pp. 870-871.
4. McDonald J.M., Berbaum K., Bennett D.L., et. al.: Radiology residency call: residents’ perceptions of the on-call experience. J Am Coll Radiol 2005; 2: pp. 932-938.
5. Ojutiku O., Haramati L.B., Rakoff S., et. al.: Radiology residents’ on-call interpretation of chest radiographs for pneumonia. Acad Radiol 2005; 12: 658–164
6. Carney E., Kempf J., DeCarvalho V., et. al.: Preliminary interpretations of after-hours CT and sonography by radiology residents versus final interpretations by body imaging radiologists at a level 1 trauma center. AJR Am J Roentgenol 2003; 181: pp. 367-373.
7. Erly W.K., Berger W.G., Krupinski E., et. al.: Radiology resident evaluation of head CT scan orders in the emergency department. Am J Neuroradiol 2002; 23: pp. 103-107.
8. Lal N.R., Murray U.M., Eldevik O.P., et. al.: Clinical consequences of misinterpretations of neuroradiologic CT scans by on-call radiology residents. Am J Neuroradiol 2000; 21: pp. 124-129.
9. Wechsler R.J., Spettell C.M., Kurtz A.B., et. al.: Effects of training and experience in interpretation of emergency body CT scans. Radiology 1996; 199: pp. 717-720.
10. Eng J., Mysko W.K., Weller G.E., et. al.: Interpretation of emergency department radiographs: a comparison of emergency medicine physicians with radiologists, residents with faculty, and film with digital display. AJR Am J Roentgenol 2000; 175: pp. 1233-1238.
11. Cascade P.N., Kazerooni E.A., Gross B.H., et. al.: Evaluation of competence in the interpretation of chest radiographs. Acad Radiol 2001; 8: pp. 315-321.
12. Gatt M.E., Spectre G., Paltiel O., et. al.: Chest radiographs in the emergency department: is the radiologist really necessary?. Postgrad Med J 2003; 79: pp. 214-217.
13. Erly W.K., Ashdown B.C., Lucio R.W., et. al.: Evaluation of emergency CT scans of the head: is there a community standard?. AJR Am J Roentgenol 2003; 180: pp. 1727-1730.