
Rationale and Objectives
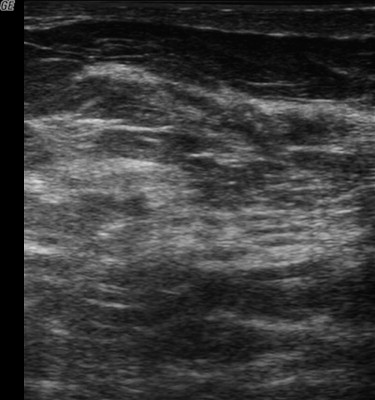
The aim of this study was to determine the sonographic visibility of implanted collagen-based breast biopsy marker clips in the clinic and operating room.
Materials and Methods
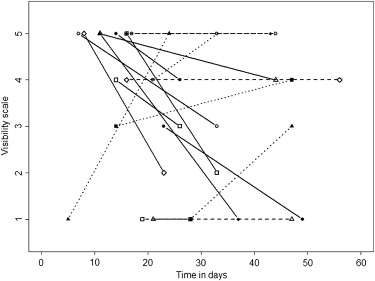
Female patients aged ≥18 years who presented for preoperative surgical evaluation within 4 weeks of ultrasound-guided breast biopsy and collagen-based marker clip placement were eligible for this pilot study. The sonographic visibility of the marker clips was rated from 1 (not visible) to 5 (clearly visible) by surgeons at the preoperative appointment, by radiologists at wire localization, and by surgeons in the operating room. Visibility was considered inadequate for values of 1 or 2 and adequate for values of 3, 4, or 5. The data were compared using Wilcoxon’s signed-rank test for paired differences across physician (radiologist vs surgeon), time (preoperative visit vs day of surgery), and target (lesion vs clip).
Results
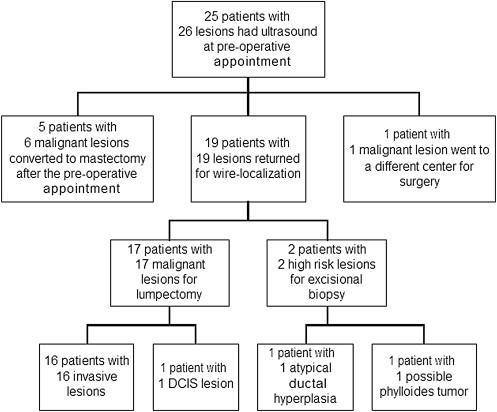
Twenty-five patients with 26 lesions were enrolled, and 19 patients returned for all imaging procedures. The mean lesion size was 12 mm (range, 5–24 mm). Adequate marker clip visibility assessed by the surgeons decreased from 80% (20 of 25) at the preoperative appointment to 65% (11 of 17) in the operating room, but the difference was not significant ( P = .27). Visibilities of the lesions and clips were similar at the preoperative appointment ( P = .61), but the clips were significantly less visible on the day of operation ( P = .03).
Conclusion
The sonographic visibility of collagen-based marker clips is variable and likely decreases over time but may be adequate to guide intraoperative surgical excision in many cases.
Breast cancer is the most common major cancer among women in the United States. It is estimated that approximately 180,000 women will be diagnosed with breast cancer, and 40,000 die from the disease annually. On the basis of rates from 2003 to 2005, 12.0% of women alive today will be diagnosed with cancer of the breast at some time during their lifetimes . Whether initially presenting in asymptomatic patients in screening mammography programs or in symptomatic patients who undergo diagnostic imaging evaluation, breast cancers are typically confirmed with image-guided tissue sampling prior to surgical excision.
It is common clinical practice for radiologists to place metallic clips in suspicious lesions at the time of a biopsy to permit localization under mammographic guidance if surgical resection is later indicated . Such image-guided wire localization is performed for nonpalpable lesions to facilitate surgical excision when breast conservation is desired. Wire localization is an invasive procedure that requires local anesthetic and needle insertion under imaging guidance before the patient is taken to the operating room. This intervention, although vital to the success of the surgical procedure, can be challenging to patients. Potential issues of preoperative localization include patient pain, discomfort, and vasovagal episodes as well as potential operating room delays.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Case Selection
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Study Procedures
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Comparison of Visibility Rankings of the Clips and Lesions Using Wilcoxon’s Signed-Rank Test
Visibility Comparison Number of Paired Values Median Difference (Range) Wilcoxon’s Signed-Rank Test P Value Surgeons: preoperative appointment vs operating room Marker clip 17 0 (−4 to 4) .27 Lesion 11 0 (−1 to 4) .43 Day of surgery: radiologists vs surgeons Marker clip 16 1 (−4 to 4) .22 Lesion 13 0 (−3 to 1) .28 Surgeons: marker clip vs lesion Preoperative appointment 14 0 (−3 to 1) .61 Operating room 16 1 (−3 to 4) .03 ∗
A two-sided P value of .05 was considered significant. Complete data were not acquired in some cases.
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Summary of Prior Studies of Intraoperative Ultrasound Localization of Masses
Study Number of Patients Number of Lesions Number of Cancers Ultrasound Localization Sensitivity Rifkin et al (1988) ‡ 45 52 3 52/52 (100%) Schwartz et al (1988) ‡ 95 105 9 92/105 (88%) Fornage et al (1994) ∗ 26 26 10 24/26 (92%) Harlow et al (1999) ∗ 62 65 65 65/65 (100%) Paramo et al (1999) ∗ 15 15 3 15/15 (100%) Rahusen et al (1999) ∗ 19 20 19 19/20 (95%) Snider and Morrison (1999) † 29 29 22 29/29 (100%) Smith et al (2000) ‡ 77 81 25 81/81 (100%) Moore et al (2001) § 27 27 27 27/27 (100%) Rahusen et al (2002) † 27 27 27 27/27 (100%) Kaufman et al (2003) || 100 101 101 101/101 (100%) Bennett et al (2005) ∗ 103 115 48 115/115 (100%) Ngo et al (2007) ∗ 70 70 70 67/70 (96%)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. National Cancer Institute : SEER cancer statistics review 1975-2004: Table IV-17: female breast cancer (invasive). Available at: http://seer.cancer.gov/csr/1975_2004/results_single/sect_04_table.17.pdf Accessed November 3, 2009
2. Burbank F., Forcier N.: Tissue marking clip for stereotactic breast biopsy: initial placement accuracy, long-term stability, and usefulness as a guide for wire localization. Radiology 1997; 205: pp. 407-415.
3. Dash N., Chafin S.H., Johnson R.R., et. al.: Usefulness of tissue marker clips in patients undergoing neoadjuvant chemotherapy for breast cancer. AJR Am J Roentgenol 1999; 173: pp. 911-917.
4. Guenin M.A.: Clip placement during sonographically guided large-core breast biopsy for mammographic-sonographic correlation. AJR Am J Roentgenol 2000; 175: pp. 1053-1055.
5. Margolin F.R., Jacobs R.P., Denny S.R., et. al.: Clip placement after sonographically guided percutaneous breast biopsy. Breast J 2003; 9: pp. 226-230.
6. Margolin F.R., Kaufman L., Denny S.R., et. al.: Metallic marker placement after stereotactic core biopsy of breast calcifications: comparison of two clips and deployment techniques. AJR Am J Roentgenol 2003; 181: pp. 1685-1690.
7. Oh J.L., Nguyen G., Whitman G.J., et. al.: Placement of radiopaque clips for tumor localization in patients undergoing neoadjuvant chemotherapy and breast conservation therapy. Cancer 2007; 110: pp. 2420-2427.
8. Perlet C., Sittek H., Reiser M., et. al.: Clip marker placement following MR-guided vacuum biopsy of the breast [article in German]. Radiologe 2005; 45: pp. 230-236.
9. Reynolds H.E.: Marker clip placement following directional, vacuum-assisted breast biopsy. Am Surg 1999; 65: pp. 59-60.
10. Sittek H., Heske N., Kessler M., et. al.: O-twist marker for post-interventional marking in imaging of suspected breast lesions [article in German]. Radiologe 2005; 45: pp. 223-229.
11. Uematsu T.: Commercially available titanium clip placement following a sonographically guided core needle biopsy of the breast. Breast J 2007; 13: pp. 624-626.
12. Viehweg P., Fabel K., Petzold A., et. al.: O-Twist Marker for marking breast cancer under neoadjuvant chemotherapy—first results [article in German]. Rofo 2007; 179: pp. 1055-1060.
13. Homer M.J.: Localization of transected wire. AJR Am J Roentgenol 1991; 157: pp. 645.
14. Helvie M.A., Ikeda D.M., Adler D.D.: Localization and needle aspiration of breast lesions: complications in 370 cases. AJR Am J Roentgenol 1991; 157: pp. 711-714.
15. Davis P.S., Wechsler R.J., Feig S.A., et. al.: Migration of breast biopsy localization wire. AJR Am J Roentgenol 1988; 150: pp. 787-788.
16. Mitus J., Kolodziejski L., Dyczek S., et. al.: Localization wire migrating into the hilum of the lung during wire-guided breast biopsy. Breast J 2004; 10: pp. 165-166.
17. van Susante J.L., Barendregt W.B., Bruggink E.D.: Migration of the guide-wire into the pleural cavity after needle localization of breast lesions. Eur J Surg Oncol 1998; 24: pp. 446-448.
18. Owen A.W., Kumar E.N.: Migration of localizing wires used in guided biopsy of the breast. Clin Radiol 1991; 43: pp. 251.
19. Jackman R.J., Marzoni F.A.: Needle-localized breast biopsy: why do we fail?. Radiology 1997; 204: pp. 677-684.
20. Norton L.W., Zeligman B.E., Pearlman N.W.: Accuracy and cost of needle localization breast biopsy. Arch Surg 1988; 123: pp. 947-950.
21. Chadwick D.R., Shorthouse A.J.: Wire-directed localization biopsy of the breast: an audit of results and analysis of factors influencing therapeutic value in the treatment of breast cancer. Eur J Surg Oncol 1997; 23: pp. 128-133.
22. Acosta J.A., Greenlee J.A., Gubler K.D., et. al.: Surgical margins after needle-localization breast biopsy. Am J Surg 1995; 170: pp. 643-646.
23. Yim J.H., Barton P., Weber B., et. al.: Mammographically detected breast cancer. Benefits of stereotactic core versus wire localization biopsy. Ann Surg 1996; 223: pp. 688-700.
24. Liberman L., Kaplan J., Van Zee K.J., et. al.: Bracketing wires for preoperative breast needle localization. AJR Am J Roentgenol 2001; 177: pp. 565-572.
25. Besic N., Zgajnar J., Hocevar M., et. al.: Breast biopsy with wire localization: factors influencing complete excision of nonpalpable carcinoma. Eur Radiol 2002; 12: pp. 2684-2689.
26. Florentine B.D., Kirsch D., Carroll-Johnson R.M., et. al.: Conservative excision of wire-bracketed breast carcinomas: a community hospital’s experience. Breast J 2004; 10: pp. 398-404.
27. Kirstein L.J., Rafferty E., Specht M.C., et. al.: Outcomes of multiple wire localization for larger breast cancers: when can mastectomy be avoided?. J Am Coll Surg 2008; 207: pp. 342-346.
28. Canavese G., Catturich A., Vecchio C., et. al.: Pre-operative localization of non-palpable lesions in breast cancer by charcoal suspension. Eur J Surg Oncol 1995; 21: pp. 47-49.
29. Gennari R., Galimberti V., De Cicco C., et. al.: Use of technetium-99 m-labeled colloid albumin for preoperative and intraoperative localization of nonpalpable breast lesions. J Am Coll Surg 2000; 190: pp. 692-699.
30. Gittleman M.A.: Single-step ultrasound localization of breast lesions and lumpectomy procedure. Am J Surg 2003; 186: pp. 386-390.
31. Rifkin M.D., Schwartz G.F., Pasto M.E., et. al.: Ultrasound for guidance of breast mass removal. J Ultrasound Med 1988; 7: pp. 261-263.
32. Schwartz G.F., Goldberg B.B., Rifkin M.D., et. al.: Ultrasonography: an alternative to x-ray-guided needle localization of nonpalpable breast masses. Surgery 1988; 104: pp. 870-873.
33. Fornage B.D., Ross M.I., Singletary S.E., et. al.: Localization of impalpable breast masses: value of sonography in the operating room and scanning of excised specimens. AJR Am J Roentgenol 1994; 163: pp. 569-573.
34. Harlow S.P., Krag D.N., Ames S.E., et. al.: Intraoperative ultrasound localization to guide surgical excision of nonpalpable breast carcinoma. J Am Coll Surg 1999; 189: pp. 241-246.
35. Paramo J.C., Landeros M., McPhee M.D., et. al.: Intraoperative ultrasound-guided excision of nonpalpable breast lesions. Breast J 1999; 5: pp. 389-394.
36. Rahusen F.D., Taets van Amerongen A.H., van Diest P.J., et. al.: Ultrasound-guided lumpectomy of nonpalpable breast cancers: A feasibility study looking at the accuracy of obtained margins. J Surg Oncol 1999; 72: pp. 72-76.
37. Snider H.C., Morrison D.G.: Intraoperative ultrasound localization of nonpalpable breast lesions. Ann Surg Oncol 1999; 6: pp. 308-314.
38. Smith L.F., Rubio I.T., Henry-Tillman R., Korourian S., Klimberg V.S.: Intraoperative ultrasound-guided breast biopsy. Am J Surg 2000; 180: pp. 419-423.
39. Moore M.M., Whitney L.A., Cerilli L., et. al.: Intraoperative ultrasound is associated with clear lumpectomy margins for palpable infiltrating ductal breast cancer. Ann Surg 2001; 233: pp. 761-768.
40. Rahusen F.D., Bremers A.J., Fabry H.F., et. al.: Ultrasound-guided lumpectomy of nonpalpable breast cancer versus wire-guided resection: a randomized clinical trial. Ann Surg Oncol 2002; 9: pp. 994-998.
41. Kaufman C.S., Jacobson L., Bachman B., et. al.: Intraoperative ultrasonography guidance is accurate and efficient according to results in 100 breast cancer patients. Am J Surg 2003; 186: pp. 378-382.
42. Bennett I.C., Greenslade J., Chiam H.: Intraoperative ultrasound-guided excision of nonpalpable breast lesions. World J Surg 2005; 29: pp. 369-374.
43. Ngo C., Pollet A.G., Laperrelle J., et. al.: Intraoperative ultrasound localization of nonpalpable breast cancers. Ann Surg Oncol 2007; 14: pp. 2485-2489.
44. Kaufman C.S., Jacobson L., Bachman B., et. al.: Intraoperative ultrasound facilitates surgery for early breast cancer. Ann Surg Oncol 2002; 9: pp. 988-993.