
Rationale and Objectives
It is well known that synchronous cancers (incidence, 2%–11%) and polyps (incidence, 12%–58%) occur in patients with colorectal cancer. Magnetic resonance colonography (MRC) seems like the obvious choice as a diagnostic tool in preoperative evaluation, because it is noninvasive, and most of the colon can be evaluated. Furthermore, it has higher patient acceptance, and no sedation or radiation is used. The purpose of this study was to determine the feasibility of performing MRC preoperatively in an everyday clinical situation in a group of patients who were not offered a full conventional colonoscopy or in whom full conventional colonoscopy was not possible.
Materials and Methods
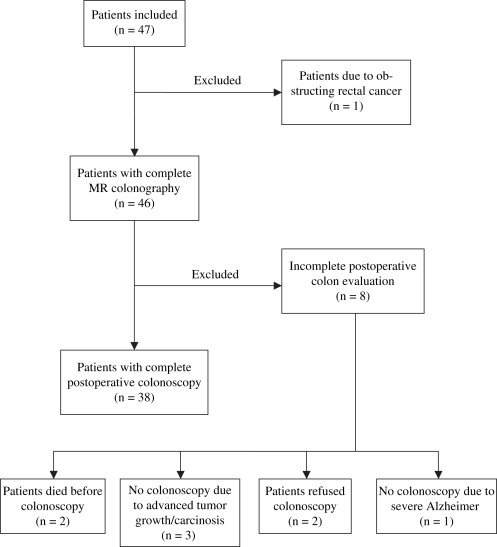
In a 13-month period, 47 patients diagnosed with rectal or sigmoid colon cancer scheduled for operation were included in the study. MRC was performed with bowel purgation either the night before surgery or as ambulatory MRC the week before surgery.
Results
Full MRC was performed in 98% of the patients. In four patients, 12 synchronous lesions (one cancer, two plaques of carcinosis, and nine adenomas) were found. One flat adenoma and five small polyps were missed by MRC and perioperative palpation but found on postoperative colonoscopy. The findings resulted in altered operative strategies in three patients.
Conclusion
This study shows the feasibility and potential gain of preoperative MRC in patients with sigmoid colon cancer or rectal cancer.
Synchronous cancers and polyps in the colon are well-known occurrences in patients with colorectal cancer. Synchronous lesions have been described numerous times in the literature, with varying incidences of 2% to 11% for cancers and 12% to 58% for polyps . Thus, the widespread recommendation for full colonic evaluation preoperatively with conventional colonoscopy (CC) seems only sensible and is aimed at reducing morbidity and mortality.
Magnetic resonance (MR) colonography (MRC) was first described in 1997 by Luboldt et al , and with its noninvasive nature and per patient high sensitivity for MRC with bowel purgation close to 100% for lesions >10 mm , many have begun regarding MRC as the diagnostic tool of the future. Thus, MRC seems like the obvious choice as a diagnostic tool in preoperative evaluation. It is noninvasive (fewer complications), and because of the method of using water or air for colon distention, most of the colon can be evaluated (fewer incomplete evaluations) . Furthermore, MRC has higher patient acceptance (compliance), and no sedation or radiation is used . So far, only one smaller experimental study has been conducted concerning the preoperative evaluation of patients with colorectal cancer using MRC , but several studies using computed tomographic colonography have been published . Although not directly comparable, all of the studies have concluded that MRC or computed tomographic colonography is feasible and useful in evaluating the entire colon preoperatively, especially in patients with occlusive carcinomas.
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Patient Preparation for MRC
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MR Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conventional Colonoscopy
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Magnetic Resonance Colonography
Get Radiology Tree app to read full this article<



Get Radiology Tree app to read full this article<
Perioperative Findings
Get Radiology Tree app to read full this article<
Conventional Colonoscopy
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Synchronous Polyps Missed By Pre-, Peri-, and Post-operative Colon Evaluation
Cancer Polyp Size Location Preoperative Endoscopy MRC Surgery Postoperative Colonoscopy Nonobstructing rectal cancer 8 mm 11 cm above cancer Missed Missed Missed Visualized Obstructing sigmoid cancer 4 × 10 mm flat polyp 10 cm below cancer Missed Missed Missed Visualized Obstructing rectal cancer 7 mm Transverse colon NV Missed Missed Visualized 7 mm Descending colon NV Missed Missed Visualized Obstructing rectum cancer 5 mm Caecum NV Missed Missed Visualized ∗ 4 mm Caecum NV Missed Missed Visualized ∗
NV, location not visualized because of incomplete colon evaluation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Incidence of Synchronous Cancers and Polyps in Earlier Studies
Study Design Number of Patients Synchronous Cancers Synchronous Polyps Cunliffe et al Prospective 223 11% — Isler et al Retrospective 98 7% 28% Nikoloudis et al Retrospective 283 2% 12% Adloff et al Retrospective 1037 2% — Maxfield Retrospective 90 4% — Askew et al Prospective 85 7% 27% Arenas et al Retrospective 235 5% 30% Langevin and Nivatvongs Prospective 166 5% 27% (>5 mm) Reilly et al Prospective 157 8% — Tate et al Retrospective 130 6% — Kimura et al Retrospective 358 5% 26% Kim and Park Retrospective 265 5% 28% Demetriades et al Retrospective 307 — 24% Pagana et al Retrospective 185 7% 26%
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Adloff M., Arnaud J.P., Bergamaschi R., Schloegel M.: Synchronous carcinoma of the colon and rectum: prognostic and therapeutic implications. Am J Surg 1989; 157: pp. 299-302.
2. Cunliffe W.J., Hasleton P.S., Tweedle D.E., Schofield P.F.: Incidence of synchronous and metachronous colorectal carcinoma. Br J Surg 1984; 71: pp. 941-943.
3. Isler J.T., Brown P.C., Lewis F.G., Billingham R.P.: The role of preoperative colonoscopy in colorectal cancer. Dis Colon Rectum 1987; 30: pp. 435-439.
4. Nikoloudis N., Saliangas K., Economou A., et. al.: Synchronous colorectal cancer. Tech Coloproctol 2004; 8: pp. s177-s179.
5. Achiam MP, Burgdorf SK, Wilhelmsen M, Alamili M, Rosenberg J. Inadequate preoperative colonic evaluation for synchronous colorectal cancer. Scand J Surg. In press.
6. Bat L., Neumann G., Shemesh E.: The association of synchronous neoplasms with occluding colorectal cancer. Dis Colon Rectum 1985; 28: pp. 149-151.
7. Askew A., Ward M., Cowen A.: The influence of colonoscopy on the operative management of colorectal cancer. Med J Aust 1986; 145: pp. 254-255.
8. Maxfield R.G.: Colonoscopy as a routine preoperative procedure for carcinoma of the colon. Am J Surg 1984; 147: pp. 477-480.
9. Luboldt W., Bauerfeind P., Steiner P., Fried M., Krestin G.P., Debatin J.F.: Preliminary assessment of three-dimensional magnetic resonance imaging for various colonic disorders. Lancet 1997; 349: pp. 1288-1291.
10. Ajaj W., Pelster G., Treichel U., et. al.: Dark lumen magnetic resonance colonography: comparison with conventional colonoscopy for the detection of colorectal pathology. Gut 2003; 52: pp. 1738-1743.
11. Lauenstein T.C., Goehde S.C., Ruehm S.G., Holtmann G., Debatin J.F.: MR colonography with barium-based fecal tagging: initial clinical experience. Radiology 2002; 223: pp. 248-254.
12. Pappalardo G., Polettini E., Frattaroli F.M., Casciani E., D’Orta C., D’Amato M., Gualdi G.F.: Magnetic resonance colonography versus conventional colonoscopy for the detection of colonic endoluminal lesions. Gastroenterology 2000; 119: pp. 300-304.
13. So N.M., Lam W.W., Mann D., Leung K.L., Metreweli C.: Feasibility study of using air as a contrast medium in MR colonography. Clin Radiol 2003; 58: pp. 555-559.
14. Achiam MP, Logager VB, Chabanova E, Eegholm B, Thomsen HS, Rosenberg J. Diagnostic accuracy of MR colonography with fecal tagging. Abdom Imaging. In press.
15. Ajaj W., Lauenstein T.C., Pelster G., et. al.: MR colonography in patients with incomplete conventional colonoscopy. Radiology 2005; 234: pp. 452-459.
16. Achiam MP, Logager V, Chabanova E, Thomsen HS, Rosenberg J. Patient acceptance of MR colonography with improved fecal tagging versus conventional colonoscopy. Eur J Radiol. In press.
17. Meier C., Wildermuth S.: Feasibility and potential of MR-colonography for evaluating colorectal cancer. Swiss Surg 2002; 8: pp. 21-24.
18. Fenlon H.M., McAneny D.B., Nunes D.P., Clarke P.D., Ferrucci J.T.: Occlusive colon carcinoma: virtual colonoscopy in the preoperative evaluation of the proximal colon. Radiology 1999; 210: pp. 423-428.
19. Morrin M.M., Farrell R.J., Raptopoulos V., McGee J.B., Bleday R., Kruskal J.B.: Role of virtual computed tomographic colonography in patients with colorectal cancers and obstructing colorectal lesions. Dis Colon Rectum 2000; 43: pp. 303-311.
20. Campillo-Soto A., Pellicer-Franco E., Parlorio-Andres E., Soria-Aledo V., Morales-Cuenca G., Guayo-Albasini J.L.: CT colonography vs barium enema for the preoperative study of colorectal cancer in patients with incomplete colonoscopy. Med Clin (Barc) 2007; 129: pp. 725-728.
21. Chung D.J., Huh K.C., Choi W.J., Kim J.K.: CT colonography using 16-MDCT in the evaluation of colorectal cancer. AJR Am J Roentgenol 2005; 184: pp. 98-103.
22. Galia M., Midiri M., Carcione A., et. al.: Usefulness of CT colonography in the preoperative evaluation of patients with distal occlusive colorectal carcinoma. Radiol Med 2001; 101: pp. 235-242.
23. Kim J.H., Kim W.H., Kim T.I., Kim N.K., Lee K.Y., Kim K.W.: Incomplete colonoscopy in patients with occlusive colorectal cancer: usefulness of CT colonography according to tumor location. Yonsei Med J 2007; 48: pp. 934-941.
24. Neri E., Giusti P., Battolla L., et. al.: Colorectal cancer: role of CT colonography in preoperative evaluation after incomplete colonoscopy. Radiology 2002; 223: pp. 615-619.
25. Qin M.W., Pan W.D., Cong G.N., et. al.: Using of multislice helical CT colonography in patients with malignant lesions of colon. Chin Med Sci J 2005; 20: pp. 171-175.
26. Arenas R.B., Fichera A., Mhoon D., Michelassi F.: Incidence and therapeutic implications of synchronous colonic pathology in colorectal adenocarcinoma. Surgery 1997; 122: pp. 706-709.
27. Abrams J.S., Reines H.D.: Increasing incidence of right-sided lesions in colorectal cancer. Am J Surg 1979; 137: pp. 522-526.
28. Langevin J.M., Nivatvongs S.: The true incidence of synchronous cancer of the large bowel. A prospective study. Am J Surg 1984; 147: pp. 330-333.
29. Howard M.L., Greene F.L.: The effect of preoperative endoscopy on recurrence and survival following surgery for colorectal carcinoma. Am Surg 1990; 56: pp. 124-127.
30. Heald R.J., Bussey H.J.: Clinical experiences at St. Mark’s Hospital with multiple synchronous cancers of the colon and rectum. Dis Colon Rectum 1975; 18: pp. 6-10.
31. Reilly J.C., Rusin L.C., Theuerkauf F.J.: Colonoscopy: its role in cancer of the colon and rectum. Dis Colon Rectum 1982; 25: pp. 532-538.
32. Tate J.J., Rawlinson J., Royle G.T., Brunton F.J., Taylor I.: Pre-operative or postoperative colonic examination for synchronous lesions in colorectal cancer. Br J Surg 1988; 75: pp. 1016-1018.
33. Rex D.K., Rahmani E.Y., Haseman J.H., Lemmel G.T., Kaster S., Buckley J.S.: Relative sensitivity of colonoscopy and barium enema for detection of colorectal cancer in clinical practice. Gastroenterology 1997; 112: pp. 17-23.
34. Harrison M., Singh N., Rex D.K.: Impact of proximal colon retroflexion on adenoma miss rates. Am J Gastroenterol 2004; 99: pp. 519-522.
35. Heresbach D., Barrioz T., Lapalus M.G., et. al.: Miss rate for colorectal neoplastic polyps: a prospective multicenter study of back-to-back video colonoscopies. Endoscopy 2008; 40: pp. 284-290.
36. Berson L.H., Berger L.: Multiple carcinomas of the large intestine. Surg Gynecol Obstet 1945; 80: pp. 75-84.
37. Ajaj W., Ruehm S.G., Gerken G., Goyen M.: Strengths and weaknesses of dark-lumen MR colonography: clinical relevance of polyps smaller than 5 mm in diameter at the moment of their detection. J Magn Reson Imaging 2006; 24: pp. 1088-1094.
38. Hartmann D., Bassler B., Schilling D., et. al.: Colorectal polyps: detection with dark-lumen MR colonography versus conventional colonoscopy. Radiology 2006; 238: pp. 143-149.
39. Hurlstone D.P., Cross S.S., Adam I., et. al.: A prospective clinicopathological and endoscopic evaluation of flat and depressed colorectal lesions in the United Kingdom. Am J Gastroenterol 2003; 98: pp. 2543-2549.
40. Rembacken B.J., Fujii T., Cairns A., Dixon M.F., Yoshida S., Chalmers D.M., Axon A.T.: Flat and depressed colonic neoplasms: a prospective study of 1000 colonoscopies in the UK. Lancet 2000; 355: pp. 1211-1214.
41. Park D.H., Kim H.S., Kim W.H., et. al.: Clinicopathologic characteristics and malignant potential of colorectal flat neoplasia compared with that of polypoid neoplasia. Dis Colon Rectum 2008; 51: pp. 43-49.
42. Kimura T., Iwagaki H., Fuchimoto S., Hizuta A., Orita K.: Synchronous colorectal carcinomas. Hepatogastroenterology 1994; 41: pp. 409-412.
43. Kim M.S., Park Y.J.: Detection and treatment of synchronous lesions in colorectal cancer: the clinical implication of perioperative colonoscopy. World J Gastroenterol 2007; 13: pp. 4108-4111.
44. Demetriades H., Kanellos I., Blouhos K., et. al.: Synchronous polyps in patients with colorectal cancer. Tech Coloproctol 2004; 8: pp. s72-s75.
45. Pagana T.J., Ledesma E.J., Mittelman A., Nava H.R.: The use of colonoscopy in the study of synchronous colorectal neoplasms. Cancer 1984; 53: pp. 356-359.