
Rationale and Objectives
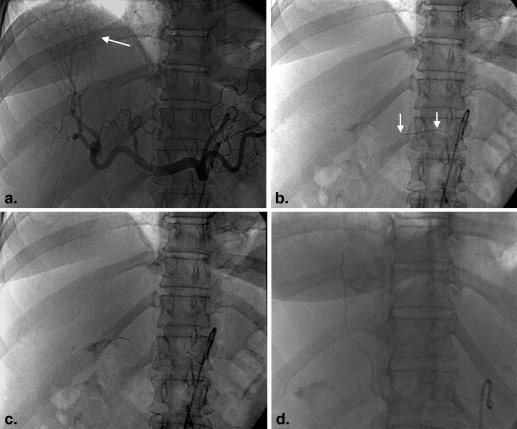
The end point of chemoembolization for hepatocellular carcinoma is qualitative. We intended to determine the feasibility of measuring intra-arterial pressure changes after chemoembolization and hypothesized that pressures would increase in the distal hepatic artery after the procedure.
Materials and Methods
Before and after chemoembolization, systemic (S) systolic and mean pressures were measured along with celiac (C), lobar (L), and distal (D) hepatic artery pressures with a pressure wire. Corrected pressures were defined as a ratio with S as the denominator to account for intraprocedural S changes. Changes in the systolic and mean corrected pressures at each location (C/S, L/S, and D/S) were evaluated using paired t tests. Pressure changes in patients with and without tumor response using the Modified Response Evaluation Criteria in Solid Tumors were also compared.
Results
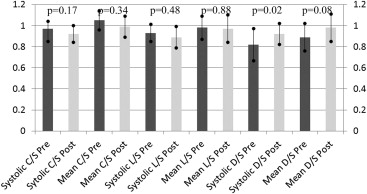
Sixteen tumors were treated in 15 patients. One patient had bilobar tumors with separate supplying arteries. The only significant pressure change was systolic D/S ( P = .02), while mean D/S approached significance ( P = .08). C/S and L/S did not change significantly after chemoembolization. Eleven of 16 patients had a complete response, whereas the other five had a partial response after chemoembolization. When comparing complete to partial responders, no changes in systolic or mean C/S, L/S, or D/S reached statistical significance (all P > .05).
Conclusions
Measuring change in hepatic artery pressures is feasible. Distal intra-arterial corrected pressures increase significantly after chemoembolization. Further study to determine the ability to predict tumor necrosis at follow-up imaging is warranted.
Chemoembolization for hepatocellular carcinoma (HCC) has gained acceptance for the treatment of Barcelona Clinic Liver Cancer intermediate-stage disease and improves survival in patients treated for palliation . Despite these clinical achievements, determining the appropriate therapeutic end point from chemoembolization remains qualitative, with completion frequently described as “relative stasis” within the treated artery . The lack of a precise end point with chemoembolization may well contribute to varying outcomes after treatment. Undertreatment can necessitate additional unwanted sessions of therapy, whereas overtreatment can result in liver decompensation .
In patients with coronary ischemia, arterial pressure measurements across stenoses with a flow-sensitive wire (PressureWire Aeris; St Jude Medical, St. Paul, MN) improve outcomes compared to decisions made by visual assessment alone . The purpose of this pilot study was to prospectively determine the feasibility of measuring intra-arterial pressure changes after chemoembolization of HCC. We hypothesized that pressures in the hepatic arteries would be measurable and that the pressures in the treated end artery would increase after chemoembolization with obstruction of distal flow. A secondary goal was to correlate changes in pressure measurements with tumor response outcomes.
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Demographic Information of the Study Patients
Demographic Patient sex, n 15 Male 11 Female 4 Median age, y 60 (range 43–79) Median tumor diameter, cm 2.3 (range 1.2–4.2) Treatment modality, n Drug eluting beads: 10 Chemotherapy/ethiodol/gelfoam: 6 Cause of cirrhosis, n Hepatitis C: 11 Alcohol: 2 Nonalcoholic steatohepatitis: 1 Unknown: 1 Child-Pugh score, n A: 11 B: 3 C: 1
Table 2
Absolute Pressures and Corrected Pressure Measurements at the Celiac, Lobar, and Distal Locations before and after Chemoembolization
Wire Location Pre-treatment Pressure: C, L, or D (mmHg) Post-treatment Pressure: C, L, or D (mmHg) Pre-treatment Corrected Pressure: C/S, L/S, or D/S Post-treatment Corrected Pressure: C/S, L/S, or D/S_P_ Value Pre vs Post Corrected Pressures Celiac systolic 118 ± 29 118 ± 31 0.97 ± 0.15 0.92 ± 0.16 .17 Celiac mean 83 ± 20 83 ± 23 1.05 ± 0.19 0.99 ± 0.21 .34 Lobar systolic 105 ± 28 115 ± 34 0.93 ± 0.18 0.89 ± 0.19 .48 Lobar mean 75 ± 18 81 ± 26 0.98 ± 0.22 0.97 ± 0.27 .88 Distal systolic 98 ± 40 116 ± 36 0.82 ± 0.29 0.92 ± 0.20 .02 Distal mean 71 ± 26 81 ± 26 0.89 ± 0.27 0.98 ± 0.26 .08
C/S, celiac pressure/systemic pressure; L/S, lobar pressure/systemic pressure; D/S, distal pressure/systemic pressure.
Of the corrected pressure ratios, only systolic pressures in the distal location demonstrated significant change after chemoembolization.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Systolic Corrected Pressures for Patients with a Complete versus Partial Response at all Locations
C/S Systolic Pre C/S Systolic Post L/S Systolic Pre L/S Systolic Post D/S Systolic Pre D/S Systolic Post_P_ Value: Complete vs Partial Response Complete response ( n = 11) 1.00 ± 0.14 0.93 ± 0.13 0.96 ± 0.14 0.91 ± 0.18 0.88 ± 0.18 0.96 ± 0.18P > .05 all measures Partial response ( n = 5) 0.92 ± 0.05 0.89 ± 0.11 0.84 ± 0.20 0.85 ± 0.12 0.68 ± 0.33 0.83 ± 0.21P > .05 all measures
C/S, celiac pressure/systemic pressure; L/S, lobar pressure/systemic pressure; D/S, distal pressure/systemic pressure.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Llovet J.M., Fuster J., Bruix J.: The Barcelona approach: diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transpl 2004; 10: pp. S115-S120.
2. Llovet J.M., Real M.I., Montana X., et. al.: Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet 2002; 359: pp. 1734-1739.
3. Lo C.M., Ngan H., Tso W.K., et. al.: Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology 2002; 35: pp. 1164-1171.
4. Brown D.B., Geschwind J.F., Soulen M.C., et. al.: Society of Interventional Radiology position statement on chemoembolization of hepatic malignancies. J Vasc Interv Radiol 2009; 20: pp. S317-S323.
5. Jin B., Wang D., Lewandowski R.J., et. al.: Chemoembolization endpoints: effect on survival among patients with hepatocellular carcinoma. AJR Am J Roentgenol 2011; 196: pp. 919-928.
6. Rhee T.K., Young J.Y., Larson A.C., et. al.: Effect of transcatheter arterial embolization on levels of hypoxia-inducible factor-1alpha in rabbit VX2 liver tumors. J Vasc Interv Radiol 2007; 18: pp. 639-645.
7. Tonino P.A., De Bruyne B., Pijls N.H., et. al.: Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med 2009; 360: pp. 213-224.
8. Gaines P.A., Schulte K.L., Muller-Hulsbeck S., et. al.: A multicentre evaluation of the Medtronic AVE Flexible Iliac Bridge Stent in the iliac arteries (the first study). Eur J Vasc Endovasc Surg 2005; 29: pp. 124-130.
9. Klein W.M., van der Graaf Y., Seegers J., et. al.: Dutch iliac stent trial: long-term results in patients randomized for primary or selective stent placement. Radiology 2006; 238: pp. 734-744.
10. Lencioni R., Llovet J.M.: Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis 2010; 30: pp. 52-60.
11. Arepally A.: Targeted drug delivery under MRI guidance. J Magn Reson Imaging 2008; 27: pp. 292-298.
12. Gaba R.C., Jin B., Wang D., et. al.: Locoregional chemoembolic delivery: prediction with transcatheter intraarterial perfusion MRI. AJR Am J Roentgenol 2012; 198: pp. 1196-1202.
13. Jin B., Wang D., Lewandowski R.J., et. al.: Quantitative 4D transcatheter intraarterial perfusion MRI for standardizing angiographic chemoembolization endpoints. AJR Am J Roentgenol 2011; 197: pp. 1237-1243.
14. Lang K., Danchenko N., Gondek K., et. al.: The burden of illness associated with hepatocellular carcinoma in the United States. J Hepatol 2009; 50: pp. 89-99.
15. Ray C.E., Battaglia C., Libby A.M., et. al.: Interventional radiologic treatment of hepatocellular carcinoma: a cost analysis from the payer perspective. J Vasc Interv Radiol 2012; 23: pp. 306-314.
16. Petruzzi N.J., Frangos A.J., Fenkel J.M., et. al.: Single-center comparison of three chemoembolization regimens for hepatocellular carcinoma. J Vasc Interv Radiol 2013; 24: pp. 266-273.