
Rationale and Objectives
The quantification of coronary calcification has established itself as a valid risk marker to predict cardiovascular events. However, data derived from cardiac multi–detector row computed tomography could demonstrate that the exclusion of coronary calcification is not synonymous with the exclusion of coronary artery disease (CAD). The aims of this retrospective analysis were to determine the prevalence of significant CAD in a symptomatic cohort with indications for invasive angiography but without coronary calcification (Agatston score 0) as assessed by multislice computed tomography and to investigate whether there were any differences in terms of risk factors between patients with and without significant CAD.
Materials and Methods
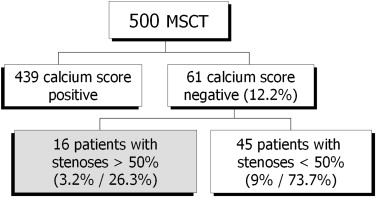
Five hundred multislice computed tomographic scans (in 371 men and 129 women) were included in the analysis. Agatston scores were determined on native scans. All patients underwent coronary angiography to detect or rule out obstructive CAD. Patients with negative calcium scoring were selected and divided into two subgroups: those without obstructive CAD and those with obstructive CAD (luminal stenoses > 50%). These subgroups were characterized in terms of clinical characteristics (age and sex) and cardiovascular risk factors (diabetes mellitus, hypertension, hyperlipoproteinemia, familial predisposition, smoking, and overweight).
Results
Sixty-one of 500 patients (12.2%) had negative calcium scores (Agatston score 0). Sixteen of these patients (26.3%, or 3.2% of the total population) had obstructive CAD according to invasive angiography. Patients with obstructive CAD were significantly older (mean age, 64 ± 9 vs 55 ± 10 years; P = .003) and were more frequently diabetic (25% vs 4%, P = .0389) than patients without obstructive CAD. There were no significant differences with regard to the other risk factors.
Conclusions
In this high-risk population, the absence of coronary calcification was not sufficient to rule out CAD. Among patients without coronary calcification, the presence of significant CAD was associated with increased age and the presence of diabetes mellitus.
Coronary artery calcification (CAC) is an independent risk factor and valid indicator for coronary artery disease (CAD). The correlation between CAC and all-cause mortality has been demonstrated in numerous studies .
Cardiac computed tomography (CT) allows calcified and noncalcified coronary plaques to be visualized noninvasively. The sensitivity to detect calcified plaques is slightly higher than the accuracy to visualize noncalcified plaques . The amount of CAC can be quantified noninvasively by electron-beam CT and multislice CT (MSCT) .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Assessment of Cardiovascular Risk Factors
Get Radiology Tree app to read full this article<
Computed Tomographic Scanners and Computed Tomographic Examinations
Get Radiology Tree app to read full this article<
Calcium Scoring
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ICA
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Patient Population
Get Radiology Tree app to read full this article<
Table 1
Characteristics of the Study Group
Characteristic Value Age (y) 63 ± 10 Men/women 371/129 Body mass index (kg/m 2 ) 28.0 ± 4.2 Number of risk factors 3.2 ± 1.2 Diabetes mellitus 116 (23.2%) Hypertension 361 (72.1%) Hyperlipidemia 373 (74.6%) Current or former smoking 81 (6.2%) Family history of coronary artery disease 235 (47.0%) Overweight 277 (55.4%)
Data are expressed as mean ± standard deviation or as number (percentage).
Get Radiology Tree app to read full this article<
Coronary Calcium Scoring
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Baseline Clinical Characteristics in Patients with and without Obstructive Coronary Artery Disease
Significant CAD No Significant CAD Variable ( n = 16) ( n = 45)P Age (y) 64 ± 9 55 ± 10 .003 Men/women 11/5 25/20 NS Hypertension 13 (81.3%) 22 (48.9%) NS Body mass index (kg/m 2 ) 29.6 ± 4 28.1 ± 5 NS Diabetes mellitus 4 (25.0%) 2 (4.4%) .0389 Family history 3 (18.8%) 22 (48.9%) NS Smoking 6 (37.5%) 14 (31.1%) NS Hyperlipidemia 13 (81.3%) 28 (62.2%) NS
Data are expressed as mean ± standard deviation or as number (percentage).
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Risk Stratification with Coronary Calcium Scoring
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Budoff M.J., Shaw L.J., Liu S.T., et. al.: Long-term prognosis associated with coronary calcification: observations from a registry of 25,253 patients. J Am Coll Cardiol 2007; 49: pp. 1860-1870.
2. Shaw L.J., Raggi P., Schisterman E., et. al.: Prognostic value of cardiac risk factors and coronary artery calcium screening for all-cause mortality. Radiology 2003; 228: pp. 826-833.
3. Leber A.W., Becker A., Knez A., et. al.: Accuracy of 64-slice computed tomography to classify and quantify plaque volumes in the proximal coronary system: a comparative study using intravascular ultrasound. J Am Coll Cardiol 2006; 47: pp. 672-677.
4. Becker C.R., Knez A., Ohnesorge B., et. al.: Visualization and quantification of coronary calcifications with electron beam and spiral computed tomography. Eur Radiol 2000; 10: pp. 629-635.
5. Georgiou D., Budoff M.J., Kaufer E., et. al.: Screening patients with chest pain in the emergency department using electron beam tomography: a follow-up study. J Am Coll Cardiol 2001; 38: pp. 105-110.
6. Hausleiter J., Meyer T., Hadamitzky M., et. al.: Prevalence of noncalcified coronary plaques by 64-slice computed tomography in patients with an intermediate risk for significant coronary artery disease. J Am Coll Cardiol 2006; 48: pp. 312-318.
7. Marwan M., Ropers D., Pflederer T., et. al.: Clinical characteristics of patients with obstructive coronary lesions in the absence of coronary calcification: an evaluation by coronary CT angiography. Heart 2009; 95: pp. 1056-1060.
8. Schröder S., Küttner A., Kopp A.F., et. al.: Noninvasive evaluation of the prevalence of noncalcified atherosclerotic plaques by multi-slice detector computed tomography: results of a pilot study. Int J Cardiol 2003; 92: pp. 151-155.
9. Achenbach S., Ulzheimer S., Baum U., et. al.: Noninvasive coronary angiography by retrospectively ECG-gated multislice spiral CT. Circulation 2000; 102: pp. 2823-2828.
10. Nieman K., Oudkerk M., Rensing B.J., et. al.: Coronary angiography with multi-slice computed tomography. Lancet 2001; 357: pp. 599-603.
11. Schröder S., Kopp A.F., Baumbach A., et. al.: Noninvasive detection and evaluation of atherosclerotic coronary plaques with multislice computed tomography. J Am Coll Cardiol 2001; 37: pp. 1430-1435.
12. Achenbach S., Moselewski F., Ropers D., et. al.: Detection of calcified and noncalcified coronary atherosclerotic plaque by contrast-enhanced, submillimeter multidetector spiral computed tomography: a segment-based comparison with intravascular ultrasound. Circulation 2004; 109: pp. 14-17.
13. Detrano R., Hsiai T., Wang S., et. al.: Prognostic value of coronary calcification and angiographic stenoses in patients undergoing coronary angiography. J Am Coll Cardiol 1996; 27: pp. 285-290.
14. Detrano R.C., Wong N.D., Doherty T.M., et. al.: Coronary calcium does not accurately predict near-term future coronary events in high-risk adults. Circulation 1999; 99: pp. 2633-2638.
15. Kennedy J., Shavelle R., Wang S., Budoff M., Detrano R.C.: Coronary calcium and standard risk factors in symptomatic patients referred for coronary angiography. Am Heart J 1998; 135: pp. 696-702.
16. Budoff M.J., Nasir K., McClelland R.L., et. al.: Coronary calcium predicts events better with absolute calcium scores than age-sex-race/ethnicity percentiles: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol 2009; 53: pp. 345-352.
17. Trabold T., Buchgeister M., Küttner A., et. al.: Abschätzung der Strahlenexposition der 16-Zeilen-Multidetektor-CT des Herzens mit retrospektivem EKG-Gating. Rofo 2003; 175: pp. 1051-1055.
18. Husmann L., Gaemperli O., Schepis T., et. al.: Accuracy of quantitative coronary angiography with computed tomography and its dependency on plaque composition: plaque composition and accuracy of cardiac CT. Int J Cardiovasc Imaging 2008; 24: pp. 895-904.
19. Brodoefel H., Reimann A., Burgstahler C., et. al.: Noninvasive coronary angiography using 64-slice spiral computed tomography in an unselected patient collective: effect of heart rate, heart rate variability and coronary calcifications on image quality and diagnostic accuracy. Eur J Radiol 2008; 66: pp. 134-141.
20. Burgstahler C., Reimann A., Drosch T., et. al.: Cardiac dual-source computed tomography in patients with severe coronary calcifications and a high prevalence of coronary artery disease. J Cardiovasc Comput Tomogr 2007; 1: pp. 143-151.
21. Küttner A., Kopp A.F., Schröder S., et. al.: Diagnostic accuracy of multidetector computed tomography coronary angiography in patients with angiographically proven coronary artery disease. J Am Coll Cardiol 2004; 43: pp. 831-839.
22. Küttner A., Beck T., Drosch T., et. al.: Diagnostic accuracy of noninvasive coronary imaging using 16-detector slice spiral computed tomography with 188 ms temporal resolution. J Am Coll Cardiol 2005; 45: pp. 123-127.
23. Tsiflikas I., Brodoefel H., Reimann A.J., et. al.: Coronary CT angiography with dual source computed tomography in 170 patients. Eur J Radiol 2010; 74: pp. 161-165.
24. Cheng V.Y., Lepor N.E., Madyoon H., et. al.: Presence and severity of noncalcified coronary plaque on 64-slice computed tomographic coronary angiography in patients with zero and low coronary artery calcium. Am J Cardiol 2007; 99: pp. 1183-1186.
25. Kelly J.L., Thickman D., Abramson S.D., et. al.: Coronary CT angiography findings in patients without coronary calcification. AJR Am J Roentgenol 2008; 191: pp. 50-55.
26. Elkeles RS. Coronary artery calcium and cardiovascular risk in diabetes. Atherosclerosis. In press.
27. Raggi P., Shaw L.J., Berman D.S., et. al.: Prognostic value of coronary artery calcium screening in subjects with and without diabetes. J Am Coll Cardiol 2004; 43: pp. 1663-1669.