
Rationale and Objectives
This study aims to determine the prevalence and predictive value of Breast Imaging Reporting and Data System (BI-RADS) 3, 4, and 5 findings on breast magnetic resonance imaging (MRI) and to evaluate the impact of study indication on the predictive value of BI-RADS categories.
Materials and Methods
This institutional review board approved, Health Insurance Portability and Accountability Act (HIPAA) compliant retrospective review of our breast MRI database from 2009 to 2011, of 5778 contrast-enhanced studies in 3360 patients was performed. At our institution, each breast receives an individual BI-RADS assessment. Breast MRI reports and electronic medical records were reviewed to obtain BI-RADS assessment, patient demographics, and outcomes. Univariate analysis was performed with Fisher exact and chi-square tests.
Results
A total of 9216 BI-RADS assessments were assigned during the study period: 7879 (85.5%) BI-RADS 1 and 2, 567 (6.2%) BI-RADS 3, 715 (7.8%) BI-RADS 4, and 55 (0.6%) BI-RADS 5 assessments. The frequency of BI-RADS 3, 4, and 5 assessments was higher in studies performed for diagnostic (7.8%, 14.6%, 1.6%, respectively) than screening (5.2%, 4.0%, 0.1%) indications ( P < 0.01). A total of 663 BI-RADS 4 and 5 lesions were biopsied with 209 (31.5%) malignant and 454 (68.5%) benign outcomes. The overall cancer rate for BI-RADS 3 findings was 1.9% (11 of 567) with no difference observed by study indication (diagnostic, 1.6%; screening, 2.3%; P = 0.76). The positive predictive value (PPV2) of BI-RADS 4 and 5 was higher for diagnostic (29.1%, 154 of 530) than for screening (22.9%, 55 of 240) indications.
Conclusions
Abnormal interpretation rates and PPV2 for MRIs performed for diagnostic indications are higher than for screening indications. Similar to mammography, breast MRI audits should be separated by study indication.
Introduction
Contrast-enhanced breast magnetic resonance imaging (MRI) is the most sensitive modality for detecting breast cancer . The modality is currently used both as an adjunct screening tool to mammography for the evaluation of asymptomatic women at high risk of breast cancer, as well as a diagnostic tool in other settings, such as assessment of the extent of the disease for known cancer diagnosis, surveillance after cancer treatment, or problem solving of inconclusive mammographic or ultrasound findings. To facilitate the increasing use of breast MRI in both the academic and community settings, the American College of Radiology (ACR) has provided recommendations for performing breast MRI in the screening and diagnostic populations and, in 2010, began an accreditation program for breast MRI facilities .
To obtain accreditation, breast MRI centers must use the ACR Breast Imaging Reporting and Data System (BI-RADS) lexicon in reporting breast MRI findings . They must be able to provide biopsy capabilities, either at their own center or a referring facility, for suspicious breast MRI findings recommended for biopsy. In addition, breast MRI centers are required to maintain a medical audit outcome program, which includes follow-up of positive BI-RADS assessments (BI-RADS 3, 4, and 5) and to provide a radiology-pathology correlation for biopsied findings on MRI .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Study Population
Get Radiology Tree app to read full this article<
Breast MR Image Acquisition and Interpretation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Collection
Get Radiology Tree app to read full this article<
Biopsy and Pathologic Assessments
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
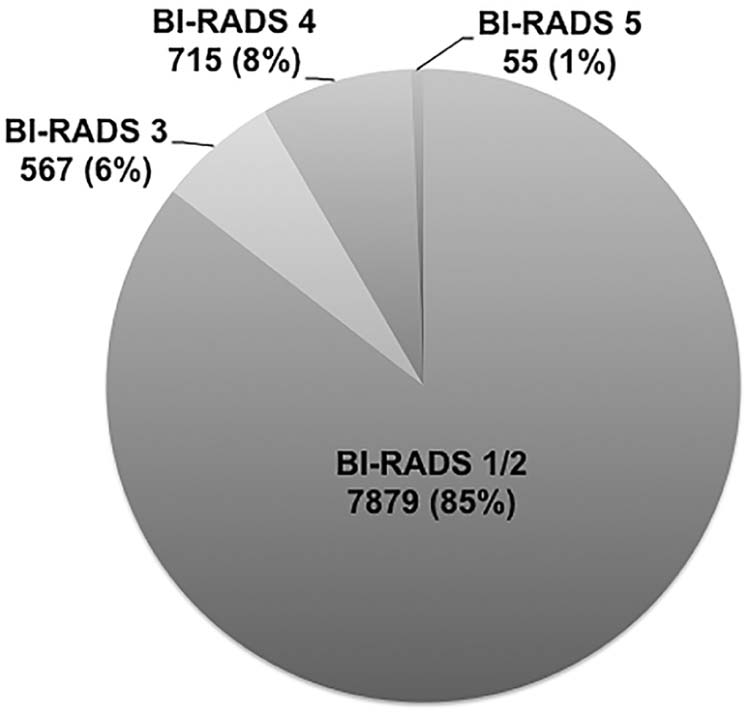
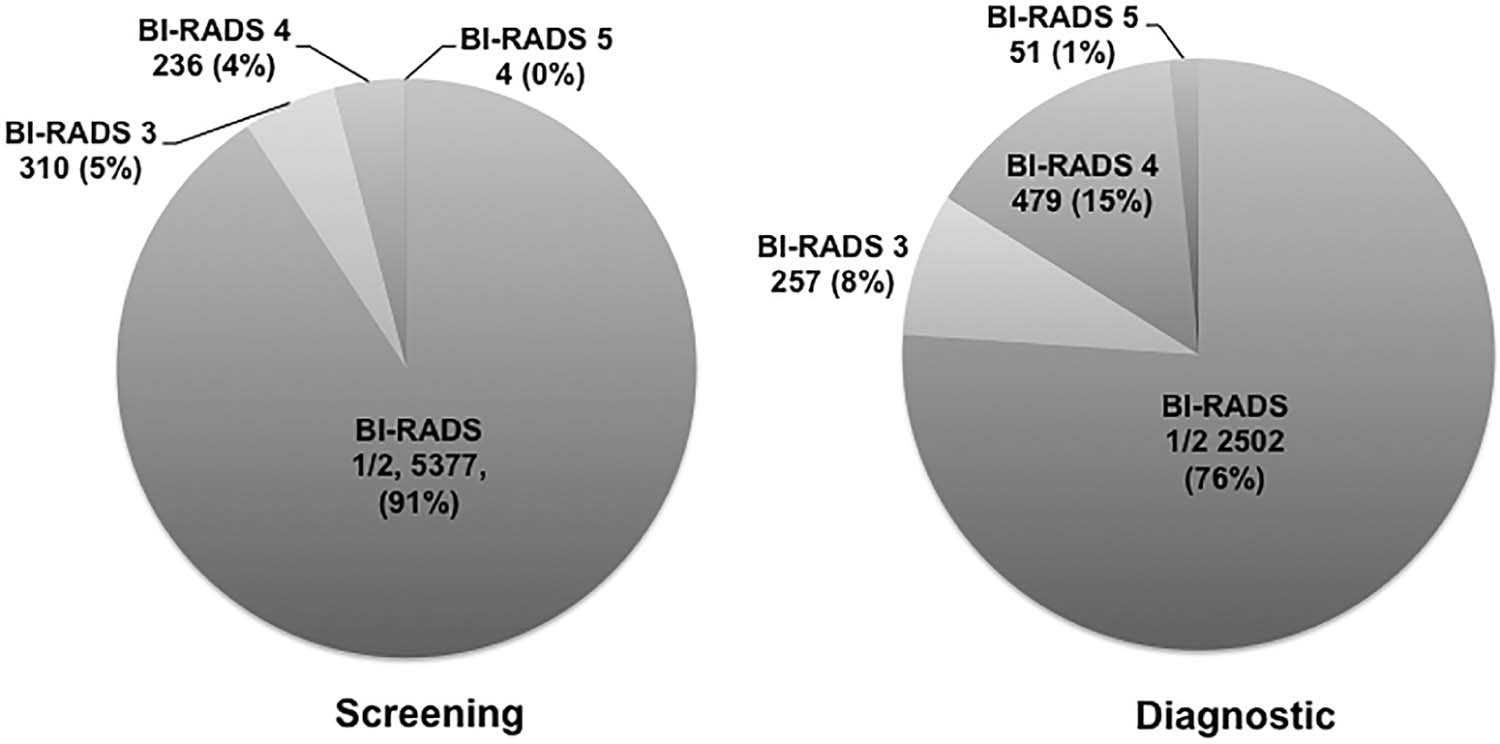
Table 1
Interpretation of Lesions Identified on Screening and Diagnostic MRI
Total Screening Diagnostic_P_ Value † Total MRIs performed 5778 3297 2481 Total lesion assessments 9216 5927 3289 Number of lesions with abnormal interpretations (BI-RADS 3, 4, and 5) 1337(14.5) 550(9.3) 787(23.9) <0.01 BI-RADS 3 567(6.2) 310(5.2) 257(7.8) <0.01 BI-RADS 4 715(7.8) 236(4.0) 479(14.6) <0.01 4A \* 214(2.3) 73(1.2) 141(4.3) <0.01 4B \* 310(3.4) 112(1.9) 198(6.0) <0.01 4C \* 77(0.8) 25(0.4) 52(1.6) <0.01 BI-RADS 5 55(0.6) 4(0.1) 51(1.6) <0.01 Abnormal interpretation rate 14.5%(1337/9216) 9.3%(550/5927) 23.9%(787/3289) <0.01
BI-RADS, Breast Imaging Reporting and Data System; MRI, magnetic resonance imaging.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Biopsy Outcomes of Lesions Identified on Screening and Diagnostic MRI
Total Screening Diagnostic_P_ Value † Total MRIs performed 5778 3297 2481 Total lesion assessments 9216 5927 3289 Biopsies performed 734(8.0) 243(4.1) 491(14.9) <0.01 BI-RADS 3 71(0.8) 39(0.7) 32(1.0) 0.11 BI-RADS 4 612(6.6) 200(3.4) 412(12.5) <0.01 4A \* 173(1.9) 56(0.9) 117(3.6) <0.01 4B \* 279(3.0) 101(1.7) 178(5.4) <0.01 4C \* 73(0.8) 23(0.4) 50(1.5) <0.01 BI-RADS 5 51(0.6) 4(0.1) 47(1.4) <0.01 Cancer diagnosis (assessment) 209(2.3) 55(0.9) 154(4.7) <0.01 BI-RADS 3 11(0.1) 7(0.1) 4(0.1) 1.00 BI-RADS 4 162(1.8) 52(0.9) 110(3.3) <0.01 4A \* 17(0.2) 7(0.1) 10(0.3) 0.07 4B \* 73(0.8) 27(0.5) 46(1.4) <0.01 4C \* 46(0.5) 12(0.2) 34(1.0) <0.01 BI-RADS 5 47(0.5) 3(0.1) 44(1.3) <0.01 Cancer detection rate per 1000 examinations \* 36.2 16.7 62.1 PPV2 ‡ 27.1%(209/770) 22.9%(55/240) 29.1%(154/530) PPV3 ‡ 31.5%(209/663) 27.0%(55/204) 33.6%(154/459)
BI-RADS, Breast Imaging Reporting and Data System; MRI, magnetic resonance imaging; PPV, positive predictive value.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Histopathologic Diagnosis of Biopsied Suspicious MRI Lesions ( n = 663)
Histopathology Screening Diagnostic Total Malignant lesions ( n = 209)n = 55(26%)n = 154(74%)n = 209 Invasive ductal carcinoma 31(56%) 68(44%) 99(47%) Invasive lobular carcinoma 3(5.5%) 21(14%) 24(11%) Ductal carcinoma in situ 16(29%) 29(19%) 45(22%) Invasive ductal and lobular carcinoma 2(4%) 13(8%) 15(7%) Other malignant lesions \* 3(5.5%) 23(15%) 26(13%) Benign lesions( n = 454)n = 146(32%)n = 308(68%)n = 454 Fibroadenoma and fibroadenomatoid changes 29(20%) 78(25%) 107(23%) Fibrocystic changes, sclerosing adenosis, columnar change, cysts, epithelial hyperplasia, microcysts, nodular adenosis, ductal ectasia 30(21%) 57(19%) 87(19%) Normal breast tissue 38(26%) 37(12%) 75(17%) Atypia including lobular neoplasia 7(5%) 63(20%) 70(15%) Radiation, inflammation, fat necrosis, fibrosis 11(7.5%) 30(9%) 41(9%) Intraductal papilloma 10(7%) 17(6%) 27(6%) Pseudoangiomatous stromal hyperplasia 8(5%) 14(5%) 22(5%) Other benign findings † 11(7.5%) 6(2%) 17(4%) Radial scar or complex sclerosing lesion 2(1%) 6(2%) 8(2%)
MRI, magnetic resonance imaging; NOS, not otherwise specified.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Lehman C.D.: Role of MRI in screening women at high risk for breast cancer. J Magn Reson Imaging 2006; 24: pp. 964-970.
2. American College of Radiology : Breast magnetic resonance imaging (MRI) accreditation program requirements.2015.American College of RadiologyReston, VA
3. Morris E.A., Comstock C.E., Lee C.H., et. al.: ACR BI-RADS magnetic resonance imaging.ACR BI-RADS atlas, breast imaging reporting and data system.2013.American College of RadiologyReston, VA:
4. Monsees B.S.: The Mammography Quality Standards Act. An overview of the regulations and guidance. Radiol Clin North Am 2000; 38: pp. 759-772.
5. Gutierrez R.L., Demartini W.B., Eby P., et. al.: Clinical indication and patient age predict likelihood of malignancy in suspicious breast MRI lesions. Acad Radiol 2009; 16: pp. 1281-1285.
6. Niell B.L., Gavenonis S.C., Motazedi T., et. al.: Auditing a breast MRI practice: performance measures for screening and diagnostic breast MRI. J Am Coll Radiol 2014; 11: pp. 883-889.
7. Lee C.I., Ichikawa L., Rochelle M.C., et. al.: Breast MRI BI-RADS assessments and abnormal interpretation rates by clinical indication in US community practices. Acad Radiol 2014; 21: pp. 1370-1376.
8. Kriege M., Brekelmans C.T.M., Boetes C., et. al.: Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med 2004; 351: pp. 427-437.
9. Kuhl C.K., Schrading S., Leutner C.C., et. al.: Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J Clin Oncol 2005; 23: pp. 8469-8476.
10. Leach M.O., Brindle K.M., Evelhoch J.L., et. al.: The assessment of antiangiogenic and antivascular therapies in early-stage clinical trials using magnetic resonance imaging: issues and recommendations. Br J Cancer 2005; 92: pp. 1599-1610.
11. Warner E., Plewes D.B., Hill K.A., et. al.: Surveillance of BRCA1 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA 2004; 292: pp. 1317-1325.
12. Sardanelli F., Podo F.: Breast MR imaging in women at high-risk of breast cancer. Is something changing in early breast cancer detection?. Eur Radiol 2007; 17: pp. 873-887.
13. Chikarmane S.A., Giess C.S., Sippo D.A., Birdwell R.L.: Lesion characteristics, malignancy rate, and follow-up of BI-RADS 3 lesions identified on breast MRI: implications for MRI interpretation and management. Radiology 2016; 280: pp. 707-715. Sep
14. Rosenberg R.D., Yankaskas B.C., Abraham L.A., et. al.: Performance benchmarks for screening mammography. Radiology 2006; 241: pp. 55-66.
15. Dee K.E., Sickles E.A.: Medical audit of diagnostic mammography examinations: comparison with screening outcomes obtained concurrently. AJR Am J Roentgenol 2001; 176: pp. 729-733.
16. Sohlich R.E., Sickles E.A., Burnside E.S., et. al.: Interpreting data from audits when screening and diagnostic mammography outcomes are combined. AJR Am J Roentgenol 2002; 178: pp. 681-686.
17. Sickles E.A.: Auditing your breast imaging practice: an evidence-based approach. Semin Roentgenol 2007; 42: pp. 211-217.
18. Kuhl C.K., Schmutzler R.K., Leutner C.C., et. al.: Breast MR imaging screening in 192 women proved or suspected to be carriers of a breast cancer susceptibility gene: preliminary results. Radiology 2000; 215: pp. 267-279.
19. DeMartini W.B., Liu F., Peacock S., et. al.: Background parenchymal enhancement on breast MRI: impact on diagnostic performance. AJR Am J Roentgenol 2012; 198: pp. W373-W380.
20. Mahoney M.C., Gatsonis C., Hanna L., et. al.: Positive predictive value of BI-RADS MR imaging. Radiology 2012; 264: pp. 51-58.
21. Lehman C.D., Gatsonis C., Kuhl C.K., et. al.: MRI evaluation of the contralateral breast in women with recently diagnosed breast cancer. N Engl J Med 2007; 356: pp. 1295-1303.
22. Liberman L., Mason G., Morris E.A., et. al.: Does size matter? Positive predictive value of MRI-detected breast lesions as a function of lesion size. AJR Am J Roentgenol 2006; 186: pp. 426-430.
23. Smith H., Chetlen A.L., Schetter S., et. al.: PPV(3) of suspicious breast MRI findings. Acad Radiol 2014; 21: pp. 1553-1562.
24. Sadowski E.A., Kelcz F.: Frequency of malignancy in lesions classified as probably benign after dynamic contrast-enhanced breast MRI examination. J Magn Reson Imaging 2005; 21: pp. 556-564.
25. Liberman L., Morris E.A., Benton C.L., et. al.: Probably benign lesions at breast magnetic resonance imaging: preliminary experience in high-risk women. Cancer 2003; 98: pp. 377-388.
26. Burnside E.S., Sickles E.A., Bassett L.W., et. al.: The ACR BI-RADS experience: learning from history. J Am Coll Radiol 2009; 6: pp. 851-860.
27. Sanders M.A., Roland L., Sahoo S.: Clinical implications of subcategorizing BI-RADS 4 breast lesions associated with microcalcification: a radiology-pathology correlation study. Breast J 2010; 16: pp. 28-31.
28. Torres-Tabanera M., Cárdenas-Rebollo J.M., Villar-Castaño P., et. al.: Analysis of the positive predictive value of the subcategories of BI-RADS(®) 4 lesions: preliminary results in 880 lesions. Radiologia 2012; 54: pp. 520-531.
29. Maltez de Almeida J.R., Gomes A.B., Barros T.P., et. al.: Subcategorization of suspicious breast lesions (BI-RADS Category 4) according to MRI criteria: role of dynamic contrast-enhanced and diffusion-weighted imaging. AJR Am J Roentgenol 2015; 205: pp. 222-231.
30. Raza S., Chikarmane S.A., Neilsen S.S., et. al.: BI-RADS 3, 4, and 5 lesions: value of US in management—follow-up and outcome. Radiology 2008; 248: pp. 773-781.