
Rationale and Objectives
Absence of coronary artery calcium (CAC) in symptomatic patients is associated with a very low risk of adverse cardiovascular events. However, patients with zero CAC may have noncalcified plaques (NCP). In this analysis, we sought to determine the prevalence and predictors of NCP in symptomatic patients with zero CAC.
Materials and Methods
Coronary computed tomography angiography (CCTA) was performed in 333 consecutive symptomatic patients (mean age 50 ± 12, 65% males) with zero CAC and no known coronary artery disease (CAD). Pretest likelihood was estimated by Framingham risk score (FRS). Independent predictors of NCP were identified using multivariate logistic regression.
Results
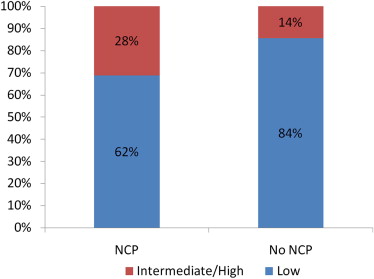
NCP was detected in 55 patients (17%) on CCTA, of which 6 patients (1.8%) had significant stenosis. In univariate analysis, patients with NCP were older (55 ± 7 vs. 50 ± 10 years, P = .009), with higher prevalence of hypertension (80% vs. 63%, P = .013). Using multivariate logistic regression, the independent predictors of NCP in this cohort were intermediate to high FRS (OR 2.3, 95%CI 1.3–4.1, P = .007), whereas baseline statin therapy was associated with lower prevalence of NCP (OR 0.38, 95%CI 0.17–0.89, P = .02).
Conclusion
Our analysis shows that nearly one in five patients with zero calcium score has NCP and one in three patients with zero calcium score and intermediate to high FRS have evidence of NCP on CCTA. The prognostic value of NCP in these patients needs further evaluation.
The role of coronary artery calcium (CAC) measurement in the diagnosis and prognosis of coronary artery disease (CAD) has undergone extensive evaluation in the last two decades. Absence of CAC is associated with a low prevalence of obstructive CAD and adverse cardiovascular events in both symptomatic and asymptomatic patients . Therefore, CAC measurement has been proposed as a “gatekeeper” for further invasive and noninvasive diagnostic testing for CAD .
In addition, The American Heart Association and American College of Cardiology expert consensus document proposed that zero CAC can be used as an effective filter before performing further diagnostic testing . CAC does not detect noncalcified plaques (NCP) that at times could cause significant stenosis . Identifying symptomatic patients with zero CAC with high likelihood of NCP may affect their management because these patients may benefit from antiatherosclerotic therapies. Also, it might preclude the need for unwarranted testing in a large number of low-risk patients preventing possible procedural complications, radiation, and contrast hazards conferred by various coronary diagnostic modalities. The prevalence of NCP in patients with zero calcium score has been very variable in the literature (ranges from 1% to 39% in different series) . Moreover, there are conflicting data regarding predictors of NCP in both symptomatic and asymptomatic patients without coronary calcification .
Get Radiology Tree app to read full this article<
Methods
Patient Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CCTA Image Acquisition
Get Radiology Tree app to read full this article<
CCTA Image Interpretation
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Clinical Characteristic of Patients with and without NCP
With NCP ( n = 55) 17% Without NCP ( n = 278) 83%P Values Age (years) 55 ± 7 50 ± 10 .009 Gender (male %) 32 (58%) 186 (67%) .02 Ethnicity African American (%) 29 (53%) 142 (51%) .09 Diabetes mellitus (%) 10 (18%) 37 (13%) .04 Dyslipidemia ∗ (%) 40 (73%) 155 (56%) .025 Hypertension (%) 44 (80%) 173 (63%) .013 FRS 4 (2–10) 2 (1–4) <.0001 Sedentary life style (%) 1 (2%) 12 (4%) .7 Smoking (%) 25 (45%) 89 (83%) .06 Body mass index (kg/m 2 ) 29 (25–35) 29 (25–35) .8 GFR (mL/min/1.73 m 2 ) 80 (70–94) 81 (70–97) .38 Statins (%) 15 (27%) 73 (26%) .86 ACEI (%) 15 (27%) 44 (16%) .44
ACEI, angiotensin-converting enzyme inhibitors; FRS, Framingham Risk Score; GFR, glomerular filtration rate; NCP, noncalcified plaque.
Get Radiology Tree app to read full this article<
Table 2
Nature of Presenting Complaint in Patients with and without NCP
Presenting Complaint With NCP ( n = 55) Without NCP ( n = 278)P Values Typical chest pain 7 (12%) 29 (11%) .59 Atypical chest pain 32 (58%) 156 (57%) .8 None cardiac chest pain 6 (11%) 37 (14%) .8 Shortness of breath only 10 (19%) 56 (18%) .7
NCP, noncalcified plaque.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Independent Predictors of NCP in Patients with Zero Calcium Score
OR 95% CI_P_ Value Statin use 0.38 0.17–0.89 .025 Intermediate/high-risk FRS 2.26 1.25–4.09 .007
FRS, Framingham Risk Score; NCP, noncalcified plaque.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Blaha M., Budoff M.J., Shaw L.J., et. al.: Absence of coronary artery calcification and all-cause mortality. JACC Cardiovasc Imaging 2009; 2: pp. 692-700.
2. Budoff M.J., Gul K.M.: Expert review on coronary calcium. Vasc Health Risk Manage 2008; 4: pp. 315-324.
3. Budoff M.J., McClelland R.L., Nasir K., et. al.: Cardiovascular events with absent or minimal coronary calcification: the Multi-Ethnic Study of Atherosclerosis (MESA). Am Heart J 2009; 158: pp. 554-561.
4. Sarwar A., Shaw L.J., Shapiro M.D., et. al.: Diagnostic and prognostic value of absence of coronary artery calcification. JACC Cardiovasc Imaging 2009; 2: pp. 675-688.
5. Palumbo A.A., Maffei E., Martini C., et. al.: Coronary calcium score as gatekeeper for 64-slice computed tomography coronary angiography in patients with chest pain: per-segment and per-patient analysis. Eur Radiol 2009; 19: pp. 2127-2135.
6. Budoff M.J., Achenbach S., Blumenthal R.S., et. al.: Assessment of coronary artery disease by cardiac computed tomography: a scientific statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation 2006; 114: pp. 1761-1791.
7. Cheng V.Y., Lepor N.E., Madyoon H., et. al.: Presence and severity of noncalcified coronary plaque on 64-slice computed tomographic coronary angiography in patients with zero and low coronary artery calcium. Am J Cardiol 2007; 99: pp. 1183-1186.
8. Hausleiter J., Meyer T., Hadamitzky M., et. al.: Prevalence of noncalcified coronary plaques by 64-slice computed tomography in patients with an intermediate risk for significant coronary artery disease. J Am Coll Cardiol 2006; 48: pp. 312-318.
9. Henneman M.M., Schuijf J.D., Pundziute G., et. al.: Noninvasive evaluation with multislice computed tomography in suspected acute coronary syndrome: plaque morphology on multislice computed tomography versus coronary calcium score. J Am Coll Cardiol 2008; 52: pp. 216-222.
10. Akram K., O’Donnell R.E., King S., et. al.: Influence of symptomatic status on the prevalence of obstructive coronary artery disease in patients with zero calcium score. Atherosclerosis 2009; 203: pp. 533-537.
11. Gottlieb I., Miller J.M., Arbab-Zadeh A., et. al.: The absence of coronary calcification does not exclude obstructive coronary artery disease or the need for revascularization in patients referred for conventional coronary angiography. J Am Coll Cardiol 2010; 55: pp. 627-634.
12. Haberl R., Tittus J., Bohme E., et. al.: Multislice spiral computed tomographic angiography of coronary arteries in patients with suspected coronary artery disease: an effective filter before catheter angiography?. Am Heart J 2005; 149: pp. 1112-1119.
13. Isma’eel H., Tellalian D., Hamirani Y.S., et. al.: Effect of obesity on coronary artery plaque using 64 slice multidetector cardiac computed tomography angiography. Int J Cardiol 2008; 140: pp. 358-360.
14. Knez A., Becker A., Leber A., et. al.: Relation of coronary calcium scores by electron beam tomography to obstructive disease in 2,115 symptomatic patients. Am J Cardiol 2004; 93: pp. 1150-1152.
15. Rubinshtein R., Gaspar T., Halon D.A., et. al.: Prevalence and extent of obstructive coronary artery disease in patients with zero or low calcium score undergoing 64-slice cardiac multidetector computed tomography for evaluation of a chest pain syndrome. Am J Cardiol 2007; 99: pp. 472-475.
16. Funabashi N., Asano M., Komuro I.: Predictors of non-calcified plaques in the coronary arteries of 242 subjects using multislice computed tomography and logistic regression models. Int J Cardiol 2007; 117: pp. 191-197.
17. Rivera J.J., Nasir K., Cox P.R., et. al.: Association of traditional cardiovascular risk factors with coronary plaque sub-types assessed by 64-slice computed tomography angiography in a large cohort of asymptomatic subjects. Atherosclerosis 2009; 206: pp. 451-457.
18. Andreini D., Pontone G., Ballerini G., et. al.: Feasibility and diagnostic accuracy of 16-slice multidetector computed tomography coronary angiography in 500 consecutive patients: critical role of heart rate. Int J Cardiovasc Imaging 2007; 23: pp. 789-801.
19. Rasouli M.L., Shavelle D.M., French W.J., et. al.: Assessment of coronary plaque morphology by contrast-enhanced computed tomographic angiography: comparison with intravascular ultrasound. Coron Artery Dis 2006; 17: pp. 359-364.
20. Schoenhagen P., Tuzcu E.M., Stillman A.E., et. al.: Non-invasive assessment of plaque morphology and remodeling in mildly stenotic coronary segments: comparison of 16-slice computed tomography and intravascular ultrasound. Coron Artery Dis 2003; 14: pp. 459-462.
21. Sosnowski M., Pysz P., Gola A., et. al.: Coronary artery visualization using a 64-row multi-slice computed tomography in unselected patients with definite or suspected coronary artery disease: a comparison with invasive coronary angiography. Cardiol J 2009; 16: pp. 413-417.
22. Achenbach S., Marwan M., Ropers D., et. al.: Coronary computed tomography angiography with a consistent dose below 1 mSv using prospectively electrocardiogram-triggered high-pitch spiral acquisition. Eur Heart J 2010; 31: pp. 340-346.
23. Diamond G.A.: A clinically relevant classification of chest discomfort. J Am Coll Cardiol 1983; 1: pp. 574-575.
24. Wilson P.W., D’Agostino R.B., Levy D., et. al.: Prediction of coronary heart disease using risk factor categories. Circulation 1998; 97: pp. 1837-1847.
25. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001; 285: pp. 2486-2497.
26. Raff G.L., Abidov A., Achenbach S., et. al.: SCCT guidelines for the interpretation and reporting of coronary computed tomographic angiography. J Cardiovasc Comput Tomogr 2009; 3: pp. 122-136.
27. Greenland P., Bonow R.O., Brundage B.H., et. al.: ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2007; 49: pp. 378-402.
28. Becker A., Knez A., Becker C., et. al.: [Prediction of serious cardiovascular events by determining coronary artery calcification measured by multi-slice computed tomography]. Dtsch Med Wochenschr 2005; 130: pp. 2433-2438.
29. Detrano R., Hsiai T., Wang S., et. al.: Prognostic value of coronary calcification and angiographic stenoses in patients undergoing coronary angiography. J Am Coll Cardiol 1996; 27: pp. 285-290.
30. Georgiou D., Budoff M.J., Kaufer E., et. al.: Screening patients with chest pain in the emergency department using electron beam tomography: a follow-up study. J Am Coll Cardiol 2001; 38: pp. 105-110.
31. Keelan P.C., Bielak L.F., Ashai K., et. al.: Long-term prognostic value of coronary calcification detected by electron-beam computed tomography in patients undergoing coronary angiography. Circulation 2001; 104: pp. 412-417.
32. Schmermund A., Stang A., Mohlenkamp S., et. al.: Prognostic value of electron-beam computed tomography-derived coronary calcium scores compared with clinical parameters in patients evaluated for coronary artery disease. Prognostic value of EBCT in symptomatic patients. Z Kardiol 2004; 93: pp. 696-705.
33. Sarwar A., Shaw L.J., Shapiro M.D., et. al.: Diagnostic and prognostic value of absence of coronary artery calcification. JACC Cardiovasc Imaging 2009; 2: pp. 675-688.
34. Leber A.W., Becker A., Knez A., et. al.: Accuracy of 64-slice computed tomography to classify and quantify plaque volumes in the proximal coronary system: a comparative study using intravascular ultrasound. J Am Coll Cardiol 2006; 47: pp. 672-677.
35. Tuzcu E.M., Kapadia S.R., Tutar E., et. al.: High prevalence of coronary atherosclerosis in asymptomatic teenagers and young adults: evidence from intravascular ultrasound. Circulation 2001; 103: pp. 2705-2710.
36. Berger J.S., Jordan C.O., Lloyd-Jones D., et. al.: Screening for cardiovascular risk in asymptomatic patients. J Am Coll Cardiol 2010; 55: pp. 1169-1177.
37. Burgstahler C., Reimann A., Beck T., et. al.: Influence of a lipid-lowering therapy on calcified and noncalcified coronary plaques monitored by multislice detector computed tomography: results of the New Age II Pilot Study. Invest Radiol 2007; 42: pp. 189-195.
38. Blaha M.J., Nasir K., Rivera J.J., et. al.: Gender differences in coronary plaque composition by coronary computed tomography angiography. Coron Artery Dis 2009; 20: pp. 506-512.
39. Nasir K., Gopal A., Blankstein R., et. al.: Noninvasive assessment of gender differences in coronary plaque composition with multidetector computed tomographic angiography. Am J Cardiol 2010; 105: pp. 453-458.
40. Budoff M.J., Nasir K., Mao S., et. al.: Ethnic differences of the presence and severity of coronary atherosclerosis. Atherosclerosis 2006; 187: pp. 343-350.