
Rationale and Objectives
Routine head computed tomography (CT) examinations often inadvertently include dental pathology which is often overlooked. The purpose of this study is to examine the prevalence of dental disease incidentally present and detected on head CT examinations, and to determine the effect of the institution of a dental disease field or macro in a standardized head CT dictation template on the rate of reporting dental disease.
Materials and Methods
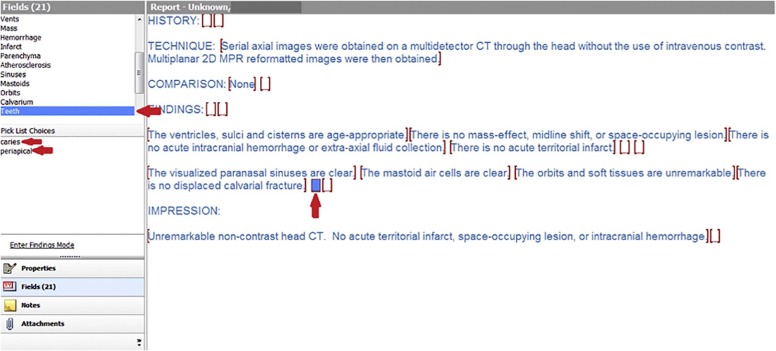
Head CT examinations were retrospectively and randomly selected from all examinations performed 6 months before, and 6 months after the institution of a dental disease field in a standardized head CT template. Dental findings were recorded from the initial finalized report. Examination images were subsequently reviewed for the presence of dental disease by two neuroradiologists who were blinded to the original reports and to each other’s findings.
Results
One hundred examinations were reviewed in the analysis. At our institution, 33% of the randomly selected head CT examinations included the level of the teeth (100/307). Dental disease was determined to be present in 40%–41% of these cases. Only 11% of the initial reports mentioned dental disease ( P < .01). Addition of a dental disease field in the dictation template resulted in no significant difference in reporting dental disease (14% vs 8%, P = .371).
Conclusions
Incidental dental disease is common and frequently underreported. Inclusion of a dental disease field in a standardized template does not significantly improve the rate of reporting dental disease.
Introduction
Computed tomography (CT) examinations of the head performed for dedicated imaging of the brain and posterior fossa-intracranial structures (referred to as “head CT” herein) are of the most common CT examinations ordered in both the inpatient and outpatient settings . A national survey estimates that head CT examinations comprise 28% of total examinations per facility compared to the second most frequently performed examination—CT of the abdomen and pelvis, which comprises 19% of total examinations . Head CT examinations are also far more frequently performed compared to dedicated CT examinations of the facial bones, orbits, and sinuses which make up 3.9% of total examinations, CT examinations of sinuses which comprise 13%, dental CT examinations which make up 0.3%, and CT examinations of the neck soft tissues which make up approximately 1% of total examinations .
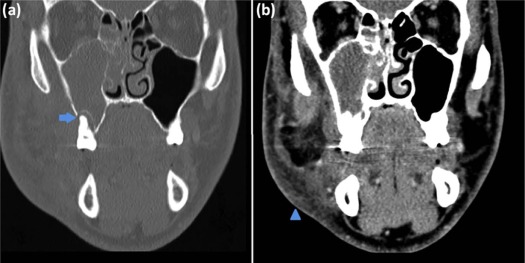
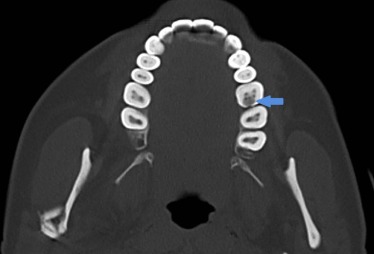
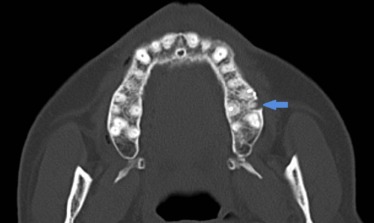
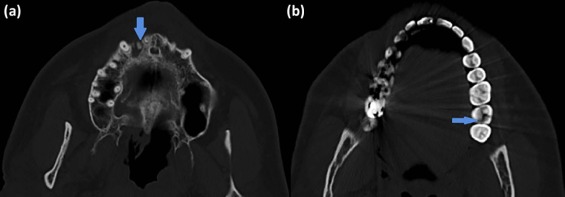
Although routine head CT examinations should not include the level of the teeth based on ideal protocol parameters, the teeth (typically maxillary but possibly both maxillary and mandibular) may be inadvertently included in the scanning field . Thus, dental disease may be incidentally seen on routine head CT examinations performed for various indications, other than dental complaints, such as headache, syncope, and trauma. Although dental disease may have implications on patient health and has been linked to cardiovascular and systemic inflammatory disease, it can be overlooked and is often underreported especially if it is in the periphery of the study such as a head CT, posing a potential blind spot for the reading radiologist . This is important because periodontal disease has been identified as an independent risk factor for coronary artery disease and stroke in certain patient populations . One study found that maternal periodontitis was associated with adverse pregnancy outcomes such as low birth weight and preeclampsia . A more recent study, which collected data on more than 65,000 postmenopausal women, found that a history of periodontal disease significantly increases the overall risk for site-specific cancers such as melanoma, breast, lung, and esophageal cancers . Although the causality of these relationships may be questioned, there is evidence that some dental disease, especially if left untreated, may lead to potentially serious pathology extending into the adjacent orbits, soft tissues, and intracranial structures, resulting in significant increase in patient morbidity and mortality . For example, odontogenic sinusitis may account for up to 12% of maxillary sinusitis, and more than 40% of deep neck infections may have a dentigerous source . There are multiple case reports of orbital cellulitis and cavernous sinus thrombosis with odontogenic origins .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Conference of Radiation Control Program Directors (CRCPD), Department of Health and Human Services : Nationwide Evaluation of X-ray Trends (NEXT). published August; Available at http://c.ymcdn.com/sites/www.crcpd.org/resource/collection/81C6DB13-25B1-4118-8600-9615624818AA/NEXT2000CT-B&W-TextEnhanced.pdf
2. American Association of Physicists in Medicine website : Routine adult head CT protocol. published March; Available at https://www.aapm.org/pubs/CTProtocols/documents/AdultRoutineHeadCT.pdf
3. Tonetti M.S.: Periodontitis and risk for atherosclerosis: an update on intervention trials. J Clin Periodontol 2009; 36: pp. 15-19.
4. Chen L., Wei B., Li J., et. al.: Association of periodontal parameters with metabolic level and systemic inflammatory markers in patients with type 2 diabetes. J Periodontol 2010; 81: pp. 364-371.
5. Humphrey L.L., Fu R., Buckley D.I., et. al.: Periodontal disease and coronary heart disease incidence: a systematic review and meta-analysis. J Gen Intern Med 2008; 23: pp. 2079-2086.
6. Grau A.J., Becher H., Ziegler C.M., et. al.: Periodontal disease as a risk factor for ischemic stroke. Stroke 2004; 35: pp. 496-501.
7. Ide M., Papapanou P.N.: Epidemiology of association between maternal periodontal disease and adverse pregnancy outcomes—systematic review. J Clin Periodontol 2013; 40: pp. 181-194.
8. Nwizu N.N., Marshall J.R., Moysich K., et. al.: Periodontal disease and incident cancer risk among postmenopausal women: results from the women’s health initiative cohort. Cancer Epidemiol Biomarkers 2017; 26: pp. 1255-1265.
9. Ide R., Hoshuyama T., Takahashi K.: The effect of periodontal disease on medical and dental costs in a middle-aged Japanese population: a longitudinal worksite study. J Periodontol 2007; 78: pp. 2120-2126.
10. Wasson J., Hopkins C., Bowdler D.: Did Ludwig’s angina kill Ludwig?. J Laryngol Otol 2006; 120: pp. 363-365.
11. Mehra P., Murad H.: Maxillary sinus disease of odontogenic origin. Otolaryngol Clin North Am 2004; 37: pp. 347-364.
12. Marioni G., Rinaldi R., Staffieri C., et. al.: Deep neck infection with dental origin: analysis of 85 consecutive cases (2000–2006). Acta Otolayrngol 2008; 128: pp. 201-206.
13. Pihlstrom B.L., Michalowicz B.S., Johnson N.W.: Periodontal diseases. Lancet 2005; 366: pp. 1809-1820.
14. Yan W., Chakrabarti R., Choong J., et. al.: Orbital cellulitis of odontogenic origin. Orbit 2005; 34: pp. 183-185.
15. Youssef O.H., Stefanyszyn M.A., Bilyk J.R.: Odontogenic orbital cellulitis. Opthal Plast Reconstr Surg 2008; 24: pp. 29-35.
16. Abdelwahhab A.A., Hussein I.A.: Cavernous sinus thrombosis as a fatal complication of a dental abscess: a case report. J Royal Med Serv 2010; 17: pp. 20-23.
17. Verma R., Junewar V., Singh R.K., et. al.: Bilateral cavernous sinus thrombosis and facial palsy as complications of dental abscess. Natl J Maxillofac Surg 2013; 4: pp. 252-255.
18. Steinklein J., Nguyen V.: Dental anatomy and pathology encountered on routine CT of the head and neck. American J Roentgenol 2013; 201: pp. 843-853.
19. Scheinfeld M.H., Shifteh K., Avery L.L., et. al.: Teeth: what radiologists should know. Radiographics 2012; 32: pp. 1927-1944.
20. Bulbul E., Yanik B., Demirpolat G.: Detection of dental pathologies in routine paranasal CT scans: a retrospective study. J Clin Diagn Res 2017; 11: pp. 17-20.
21. Caglayan F., Tozoglu U.: Incidental findings in the maxillofacial region detected by cone beam CT. Diagn Interv Radiol 2012; 18: pp. 159-163.
22. Price J.B., Thaw K.L., Tyndall D.A., et. al.: Incidental findings from cone beam computed tomography of the maxillofacial region: a descriptive retrospective study. Clin Oral Implants Res 2012; 23: pp. 1261-1268.
23. Allareddy V., Vincent S.D., Hellstein J.W., et. al.: Incidental findings on cone beam computed tomography images. Int J Dent 2012; 2012: pp. 871532.
24. Cha J.Y., Mah J., Sinclair P.: Incidental findings in the maxillofacial area with 3-dimensional cone-beam imaging. Am J Orthod Dentofacial Orthop 2007; 132: pp. 7-14.
25. Edwards R., Alsufyani N., Heo G., et. al.: The frequency and nature of incidental findings in large-field cone beam computed tomography scans of an orthodontic sample. Prog Orthod 2014; 15: pp. 37.
26. American Board of Radiology website : Noninterpretive Skills Resource Guide. Available at https://www.theabr.org/sites/all/themes/abr-media/pdf/Noninterpretive_Skills_Domain_Specification_and_Resource_Guide.pdf
27. Centers for Disease Control and Prevention website : Oral Health: preventing cavities, gum disease, tooth loss, and oral cancers at a glance. Available at https://stacks.cdc.gov/view/cdc/11862
28. Bergenholtz G., Horsted-Bindslev P., Reit C.: Apical periodontitis.Textbook of endodontology.2003.BlackwellOxford, England:pp. 113-126.
29. Dunnick N.R., Langlotz C.P.: The radiology report of the future: a summary of the 2007 intersociety conference. J Am Coll Radiol 2008; 5: pp. 626-629.
30. Kahn C.E., Langlotz C.P., Burnside E.S.: Toward best practices in radiology reporting. Radiology 2009; 252: pp. 852-856.
31. Douglas P.S., Hendel R.C., Cummings J.E., et. al.: ACCF/ACR/AHA/ASE/ASNC/HRS/NASCI/RSNA/SAIP/SCAI/SCCT/SCMR 2008 Health Policy Statement on structured reporting in cardiovascular imaging. J Am Coll Cardiol 2009; 53: pp. 76-90.