
Rationale and Objectives
To retrospectively investigate the prevalence of tracheal collapse in an emphysema cohort. The occurrence of a large degree of tracheal collapse may have important implications for the clinical management of respiratory symptoms and air trapping in patients with emphysema.
Materials and Methods
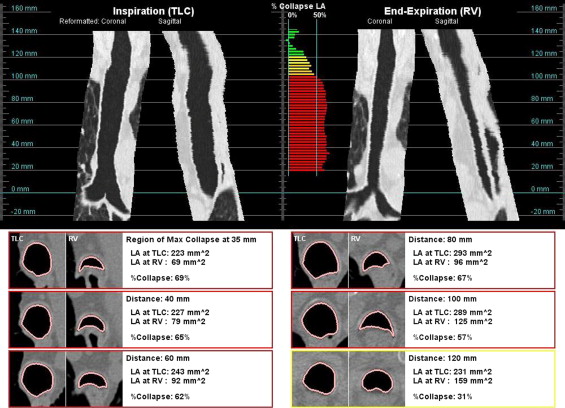
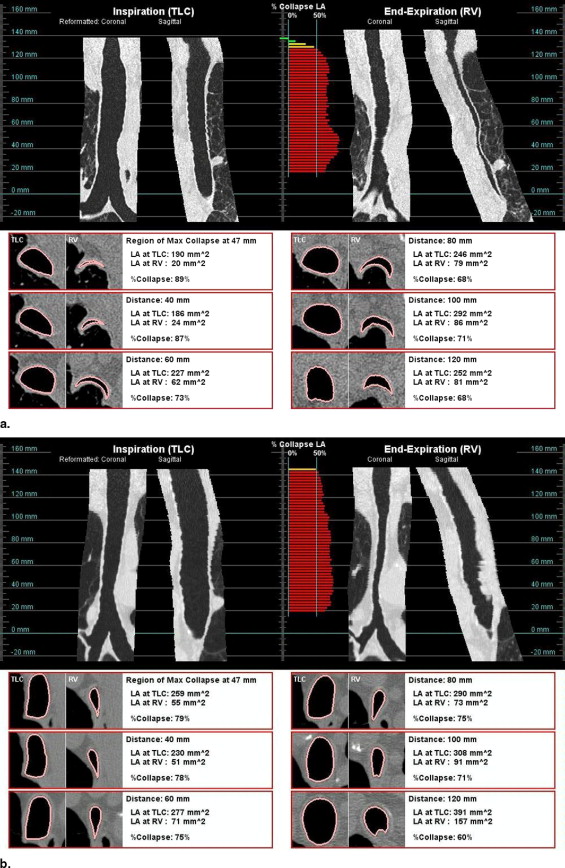
Paired full-inspiratory and end-expiratory thin-section volumetric computed tomographic scans were available for 1071 long-term smokers with clinically and physiologically confirmed emphysema. The percentage reduction in the cross-sectional tracheal luminal area from full-inspiration to end-expiration was automatically computed at 2.5-mm intervals along the centerline of the trachea using customized software.
Results
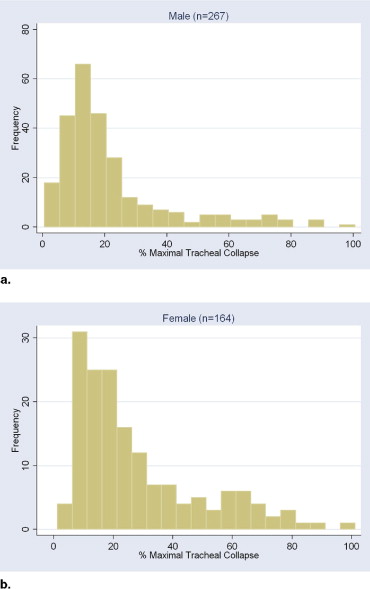
Maximal tracheal collapse did not follow a normal distribution in the emphysema cohort ( P < .0001, skewness/kurtosis tests for normality); the median collapse was 18% (intraquartile range, 11%–30%). Statistically significant differences were found in the distribution of maximal collapse by gender ( P < .005, Wilcoxon rank sum test). Overall, 10.5% of men and 17.1% of women showed evidence of tracheomalacia on the basis of the criterion of a reduction of 50% or greater in cross-sectional tracheal luminal area at end-expiration.
Conclusion
This study offers insights into the prevalence of tracheal collapse in a cohort of patients with emphysema; future work is needed to determine the possible relationship between tracheal collapse and air trapping in subjects with emphysema.
A high degree of tracheal collapse is associated with tracheomalacia, which can be diagnosed in both children and adults ( ). Tracheomalacia can be congenital or acquired; associated symptoms include dyspnea, wheeze, cough, sputum production, and hemoptysis. Investigators have suggested a correlation between tracheobronchomalacia and chronic inflammation and irritants, such as cigarette smoke ( ). Because of its nonspecific symptoms, it may be an underdiagnosed condition.
Bronchoscopy is considered the gold standard for diagnosing tracheobronchomalacia ( ); a reduction in the cross-sectional luminal area of the trachea greater than 50% is considered indicative of tracheomalacia. The reported prevalence of the disease has ranged from 1% to 13% for all subjects referred for bronchoscopic evaluation ( ) and as high as 23% for subjects with histories of chronic bronchitis ( ). The condition is commonly associated with increased age and chronic obstructive pulmonary disease ( ).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
CT Scanning Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Measurement of Tracheal Collapse
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Summary of Measurements
Variable All Subjects ⁎ Men Women_P_ Value † (n = 1071) (n = 267) (n = 164) Age (y) — 64 ± 7 62 ± 8 <0.005 Measurement LA TLC (mm 2 ) 268 ± 64 296 ± 60 221 ± 38 <0.001 LA RV (mm 2 ) 224 ± 74 253 ± 70 179 ± 54 <0.001 ΔLA avg (%) 16 ± 19 14 ± 17 19 ± 20 <0.03 ΔLA max (%) 25 ± 20 22 ± 19 28 ± 21 <0.003 Subjects with maximal tracheal collapse ≥28% 27.7% (297) 21.3% (57) 35.4% (58) ≥50% 13.4% (143) 10.5% (28) 17.1% (28) ≥70% 5.1% (55) 4.9% (13) 6.7% (11)
avg: average; LA: luminal area; max: maximal; RV: residual volume; TLC: total lung capacity.
Data are expressed as mean ± SD or as percentage (number). Significant differences were found between the genders.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Carden K.A., Boiselle P.M., Waltz D.A., Ernst A.: Tracheomalacia and tracheobronchomalacia in children and adults: an in-depth review. Chest 2005; 127: pp. 984-1005.
2. Jokinen K., Palva T., Nuutinen J.: Chronic bronchitis: a bronchologic evaluation. ORL J Otorhinolaryngol Relat Spec 1976; 38: pp. 178-186.
3. Jokinen K., Palva T., Sutinen S., Nuutinen J.: Acquired tracheobronchomalacia. Ann Clin Res 1977; 9: pp. 52-57.
4. Herzog H.: Expiratory stenosis of the trachea and great bronchi by loosening of the membraneous portion; plastic chip repair. Thoraxchirurgie 1958; 5: pp. 281-391.
5. Ikeda S., Hanawa T., Konishi T., et. al.: Diagnosis, incidence, clinicopathology and surgical treatment of acquired tracheobronchomalacia. Nihon Kyobu Shikkan Gakkai Zasshi 1992; 30: pp. 1028-1035.
6. Aquino S.L., Shepard J.O., Ginns L.C., Moore R.H., Halpern E., Grillo H.C., McLoud T.C.: Acquired tracheomalacia: detection by expiratory CT scan. J Comput Assist Tomogr 2001; 25: pp. 394-399.
7. Baroni R.H., Feller-Kopman D., Nishino M., et. al.: Tracheobronchomalacia: comparison between end-expiratory and dynamic expiratory CT for evaluation of central airway collapse. Radiology 2005; 235: pp. 635-641.
8. Boiselle P.M., Lee K.S., Ernst A.: Multidetector CT of the central airways. J Thorac Imaging 2005; 20: pp. 186-195.
9. Ferretti GR, Jankowski A, Perrin MA, et al. Multi-detector CT evaluation in patients suspected of tracheobronchomalacia: comparison of end-expiratory with dynamic expiratory volumetric acquisitions. Eur J Radiol. In press.
10. Gilkeson R.C., Ciancibello L.M., Hejal R.B., Montenegro H.D., Lange P.: Tracheobronchomalacia: dynamic airway evaluation with multidetector CT. AJR Am J Roentgenol 2001; 176: pp. 205-210.
11. Hasegawa I., Boiselle P.M., Raptopoulos V., Hatabu H.: Tracheomalacia incidentally detected on CT pulmonary angiography of patients with suspected pulmonary embolism. AJR Am J Roentgenol 2003; 181: pp. 1505-1509.
12. Heussel C., Hafner B., Lill J., Schreiber W., Thelen M., Kauczor H.U.: Paired inspiratory/expiratory spiral CT and continuous respiration cine CT in the diagnosis of tracheal instability. Eur Radiol 2001; 11: pp. 982-989.
13. Lee K.S., Sun M.R.M., Ernst A., Feller-Kopman D., Majid A., Boiselle P.M.: Comparison of dynamic expiratory CT with bronchoscopy for diagnosing airway malacia: a pilot evaluation. Chest 2007; 131: pp. 758-764.
14. Stern E.J., Graham C.M., Webb W.R., Gamsu G.: Normal trachea during forced expiration: dynamic CT measurements. Radiology 1993; 187: pp. 27-31.
15. Zhang J., Hasegawa I., Feller-Kopman D., Boiselle P.M.: Dynamic expiratory volumetric CT imaging of the central airways: comparison of standard-dose and low-dose techniques. Acad Radiol 2003; 10: pp. 719-724.
16. Zhang J., Hasegawa I., Hatabu H., Feller-Kopman D., Boiselle P.M.: Frequency and severity of air trapping at dynamic expiratory CT in patients with tracheobronchomalacia. AJR Am J Roentgenol 2004; 182: pp. 81-85.
17. Halbert R.J., Natoli J.L., Gano A., Badamgarav E., Buist A.S., Mannino D.M.: Global burden of COPD: systematic review and meta-analysis. Eur Respir J 2006; 28: pp. 523-532.
18. Goldin J.G., Brown M.S., Abtin F., et. al.: Baseline CT characteristics and image quality of the multicenter VENT study. Proc Am Thorac Soc 2007;
19. Paik D.S., Beaulieu C.F., Jeffrey R.B., Rubin G.D., Napel S.: Automated flight path planning for virtual endoscopy. Med Phys 1998; 25: pp. 629-637.
20. Wood S.A., Zerhouni E.A., Hoford J.D., Hoffman E.A., Mitzner W.: Measurement of three-dimensional lung tree structures by using computed tomography. J Appl Physiol 1995; 79: pp. 1687-1697.
21. Ochs R., Kim H.J., Goldin J., McNitt-Gray M., Brown M.: Evaluation of airway measurements in phantom parenchyma and soft tissue regions. Proc SPIE Med Imaging 2008; pp. 6916-6974.
22. Palombini B.C., Villanova C.A., Araújo E., et. al.: A pathogenic triad in chronic cough: asthma, postnasal drip syndrome, and gastroesophageal reflux disease. Chest 1999; 116: pp. 279-284.