
Rationale and Objectives
Cardiac transplant vasculopathy is the most important long-term complication of heart transplantation, with overlapping features with conventional, atherosclerotic coronary artery disease. The aim of this study was to determine the progression of coronary artery disease after heart transplantation by measuring total coronary calcium load.
Materials and Methods
After heart transplantation, 185 patients were serially examined using electron-beam computed tomography for coronary calcium load for clinical reasons. The mean time between the initial examination and the follow-up scan was 566 days (range, 126–1,436). Coronary calcium load was measured by the Agatston method, and the total calcium scores at both examinations were compared between patients taking and those not taking lipid-lowering medications (statins).
Results
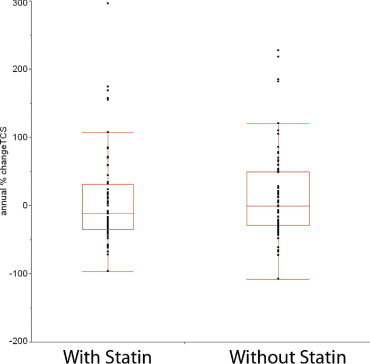
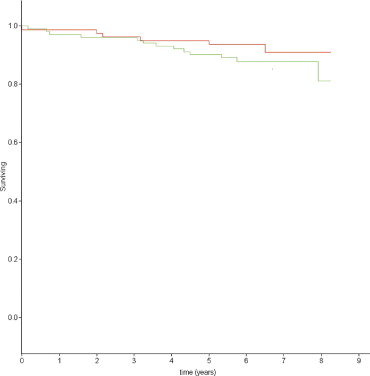
Patients not taking statins ( n = 94) displayed a median annualized percentage increase in total calcium score of 0 Agatston units, whereas patients taking at least the lowest recommended daily dose of a statin ( n = 84) displayed an annualized percentage decrease of 11 Agatston units. The difference was not statistically significant (Wilcoxon’s rank-sum test, P = .35). Only 17 patients had increases of > 24 Agatston units, and eight of them were taking statins (χ 2 test, P = .99).
Conclusion
The annual rate of progression of coronary calcium load after heart transplantation is low. In this investigation, no beneficial effects of statins could be detected.
Cardiac transplant vasculopathy (TVP) is the most important long-term complication of cardiac transplantation ( ). To diagnose TVP, intracoronary ultrasound (ICUS) has evolved as the reference technique, whereas coronary angiography fails to detect early disease ( ). Using ICUS, intimal thickening as the hallmark of TVP increases by 0.04 to 0.1 mm on average within the first year after transplantation, with important differences between medical regimens ( ). On ICUS, 75% of heart transplant recipients fulfill diagnostic criteria for TVP within the first 3 years after transplantation ( ). Although ICUS is the only clinically established method capable of detecting such subtle intimal changes, it remains an invasive method with associated risks, is costly, and is limited to the proximal coronary segments. Electron-beam computed tomography has been introduced for the noninvasive quantification of coronary calcium as a surrogate marker of coronary atherosclerosis (expressed as the total calcium score [TCS]), both in patients with conventional coronary artery disease ( ) and in heart transplant recipients ( ). Although there has been some debate about the occurrence of calcifications with TVP ( ), more recent evidence indicates that coronary calcifications do occur in TVP as well ( ).
Using electron-beam computed tomography, statins have been shown to significantly reduce the progression of coronary atherosclerosis in conventional coronary artery disease ( ). Statins reduce the progression of TVP assessed using ICUS ( ). Consequently, we hypothesized that electron-beam computed tomographic (EBCT) quantification of the coronary calcium burden in cardiac transplant recipients would reflect the progression of coronary disease and that the progression of the TCS would be less in transplant recipients treated with statins.
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Table 1
Patient Characteristics
Characteristic Value Total no. of patients 185 No. of patients with 1 follow-up EBCT study 115 No. of patients with 2 follow-up EBCT studies 57 No. of patients with 3 follow-up EBCT studies 13 Observational period (mo), range (median) 4–70 (27) Time of transplantation 1985–2000 Age at transplantation (y), mean ± SD (range) 46 ± 14 (8–67) Age at study entry (y), mean ± SD 50 ± 14 Patient gender 42 female Donor gender 51 female, 16 unknown Donor age (y), median (range) 33 (9–66) Indication for transplantation Ischemic cardiomyopathy 30 Nonischemic dilated cardiomyopathy 155
EBCT, electron-beam computed tomographic; SD, standard deviation.
Get Radiology Tree app to read full this article<
Test Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Study Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Hosenpud J.D., Bennet L.E., Keck B.M., Fiol B., Boucek M.M., Novick R.J.: The registry of the International Society for Heart and Lung Transplantation: sixteenth official report—1999. J Heart Lung Transplant 1999; 18: pp. 611-626.
2. St. Goar F.G., Pinto F.J., Alderman E.L., et. al.: Intracoronary ultrasound in cardiac transplant recipients: in vivo evidence of “angiographically silent” intimal thickening. Circulation 1992; 85: pp. 979-987.
3. Eisen H.J., Tuzcu E.M., Dorent R., et. al.: Everolimus for the prevention of allograft rejection and vasculopathy in cardiac-transplant recipients. N Engl J Med 2003; 349: pp. 847-858.
4. Ramzy D., Rao V., Brahm J., Mirikuga S., Delgado D., Ross H.J.: Cardiac allograft vasculopathy: a review. Can J Surg 2005; 48: pp. 319-327.
5. Budoff M.J., Georgiou D., Brody A., et. al.: Ultrafast computed tomography as a diagnostic modality in the detection of coronary artery disease. Circulation 1996; 93: pp. 898-904.
6. Knollmann F.D., Bocksch W., Spieglsberger S., Hetzer R., Felix R., Hummel M.: Electron-beam computed tomography in the assessment of coronary artery disease after heart transplantation. Circulation 2000; 101: pp. 2078-2082.
7. Farzaneh-Far A.: Electron-beam computed tomography in the assessment of coronary artery disease after heart transplantation (letter to the editor). Circulation 2001; 103: pp. e60.
8. Knollmann F.D., Felix R., Bocksch W., Spiegelsberger S., Hummel M., Hetzer R.: Electron-beam computed tomography in the assessment of coronary artery disease after heart transplantation (letter to the editor). Circulation 2001; 103: pp. e60.
9. Callister T.Q., Raggi P., Cooil B., Lippolis N.J., Russo D.: Effect of HMG-CoA reductase inhibitors on coronary artery disease as assessed by electron-beam computed tomography. N Engl J Med 1998; 339: pp. 1972-1978.
10. Koashigawa J.A., Katznelson S., Laks H., et. al.: Effect of pravastatin on outcomes after cardiac transplantation. N Engl J Med 1995; 333: pp. 621-627.
11. Agatston A.S., Janowitz W.R., Hildner F.J., Zusmer N.R., Viamonte M., Detrano F.: Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990; 15: pp. 827-832.
12. Budoff M.J., Lane K.L., Bakhsheshi H., et. al.: Rates of progression of coronary calcium by electron beam tomography. Am J Cardiol 2000; 86: pp. 8-11.
13. Achenbach S., Ropers D., Pohle K., et. al.: Influence of lipid-lowering therapy on the progression of coronary artery calcification. Circulation 2002; 106: pp. 1077-1082.
14. Grauhan O., Patzurek J., Hummel M., et. al.: Donor-transmitted coronary atherosclerosis. J Heart Lung Transplant 2003; 22: pp. 568-573.
15. Rumberger J.A., Kaufman L.: A Rosetta stone for coronary calcium risk stratification: Agatston, volume and mass scores in 11490 individuals. AJR Am J Roentgenol 2003; 181: pp. 743-748.
16. Schmermund A., Erbel R., Silber S.: Age and gender distribution of coronary artery calcium measured by four-slice computed tomography in 2030 persons with no symptoms of coronary artery disease. Am J Cardiol 2002; 90: pp. 168-173.
17. Yoon H.C., Emerick A.M., Hill J.A., Gjertson D.W., Goldin J.G.: Calcium begets calcium: progression of coronary artery calcification in asymptomatic subjects. Radiology 2002; 224: pp. 236-241.
18. Rahnami M., Cruz R.P., Granville D.J., McManus B.M.: Allograft vasculopathy versus atherosclerosis. Circ Res 2006; 99: pp. 801-815.
19. Li H., Tanaka K., Anzai H., et. al.: Influence of pre-existing donor atherosclerosis on the development of cardiac allograft vasculopathy and outcomes of heart transplant recipients. J Am Coll Cardiol 2006; 47: pp. 2470-2476.
20. Schmermund A., Achenbach S., Budde T., et. al.: Effect of intensive standard lipid-lowering treatment with atorvastatin on the progression of calcified coronary atherosclerosis over 12 months. Circulation 2006; 113: pp. 427-437.
21. Arad Y., Spadaro L.A., Roth M., Newstein D., Guerci A.D.: Treatment of asymptomatic adults with elevated coronary calcium scores with atorvastatin, vitamin C, and vitamin E: the St. Francis Heart Study randomized clinical trial. J Am Coll Cardiol 2005; 46: pp. 166-172.
22. Raggi P., Davidson M., Callister T.Q., et. al.: Aggressive versus moderate lipid-lowering therapy in hypercholesterolemic postmenopausal women: Beyond Endorsed Lipid Lowering With EBT Scanning (BELLES). Circulation 2005; 112: pp. 563-571.
23. Redberg R.F.: Coronary artery calcium—should we rely on this surrogate marker?. Circulation 2006; 113: pp. 336-337.