
Rationale and Objectives
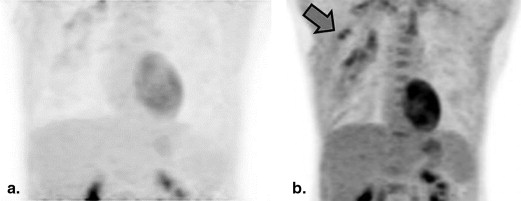
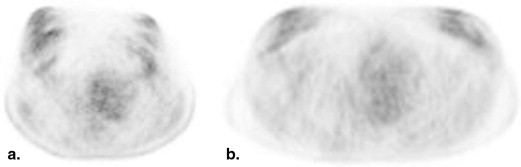
Prone 18 F fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) may have advantages for breast imaging because of improved separation of deep anatomic structures. There are limited data on whether prone and supine FDG-PET/CT provide similar information regarding breast and axillary disease in the setting of locally advanced breast cancer (LABC). The purpose of this study was to compare the information on locoregional disease distribution provided by prone versus supine FDG-PET in newly diagnosed LABC.
Materials and Methods
In an Institutional Review Board-approved prospective trial, 24 patients with newly diagnosed LABC underwent both supine and prone FDG-PET/CT at the same scanning session. Three readers performed an independent review of all scans and categorized the locoregional disease distribution as breast only (BO)-unifocal, BO-multifocal, BO-multicentric, or breast + axillary involvement. For breast + axillary disease, the readers also assessed the number of involved axillary lymph nodes. Interobserver discrepancies were resolved at a consensus reading session.
Results
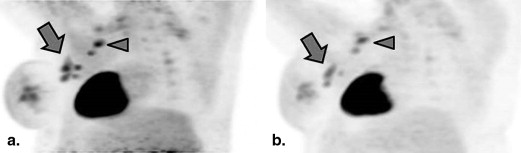
Two scanning sessions were excluded because the prone scan had omitted part of the axilla from the field of view. In the remaining 22 patients, the consensus categorization of anatomic disease distribution was concordant between prone and supine scanning in 21 patients (linear kappa 0.91, 95% confidence interval [0.79–1]). In the 16 patients with breast + axillary disease, equal numbers of involved lymph nodes were identified on prone and supine scanning in 12 patients, whereas in the remaining four patients, prone scanning resulted in a higher number of visualized lymph nodes.
Conclusions
Prone and supine FDG-PET/CT provided statistically identical information on locoregional disease distribution in LABC. However, prone scanning may perform better than supine for assessing the number of involved lymph nodes. Prone FDG-PET/CT may be useful in future clinical and research efforts, including hybrid PET–magnetic resonance imaging (MRI) applications.
Introduction
18 F fluorodeoxyglucose positron emission tomography (FDG-PET) is useful for the initial staging of locally advanced breast cancer (LABC) and for restaging breast cancer in the setting of recurrence . FDG-PET is typically performed with the patient in the supine position, but some initial studies have suggested that prone scanning may be more effective in breast cancer because of better separation of deep breast tissue, axillary, and chest wall structures . The recent introduction of hybrid PET–magnetic resonance imaging (MRI) scanners provides additional motivation for studying prone FDG-PET of the breast, as breast MRI is currently performed with the patient in the prone position, prone FDG-PET may achieve better anatomic correlation with prone breast MRI in hybrid imaging applications .
At present, there are limited data on whether prone FDG-PET provides the same information as supine FDG-PET on locoregional disease distribution in breast cancer. Although FDG-PET does not currently play a major role in the clinical assessment of tumor multifocality or axillary nodal staging, these are areas in which FDG-PET performance may improve and new FDG-PET indications may emerge, especially with the evolution of higher spatial resolution positron emission mammography and hybrid PET-MRI systems . We therefore undertook this study to compare the information offered by prone versus supine FDG-PET in the context of newly diagnosed LABC. We investigated differences between prone and supine scanning in (1) qualitative categorization of the anatomic distribution of disease and (2) assessment of the number of involved axillary lymph nodes.
Materials and methods
Patients
Get Radiology Tree app to read full this article<
FDG-PET Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Extraction
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Patient and Tumor Characteristics
Get Radiology Tree app to read full this article<
Table 1
Patient Demographic Information and Tumor Characteristics
Patient Age Diameter (Technique) Histologic Type Histologic Grade Proliferative Rate Receptor Overexpression ER PR HER2 A 48 4.2 cm (US) IMC-NST High High − − − B 46 NDM IMC-NST High Intermediate + + + C 39 10 cm (PE) ILC Low Low + + − D 56 n/a IMC-NST High Intermediate + − + E 54 9 cm (US) IMC-NST High n/a + − − F 64 2 cm (US) IMC-NST High n/a − − − G 32 2.9 cm (US) IMC-NST High High + + + H 49 1.3 cm (US) IMC-NST High Intermediate − − + I 67 2.4 cm (US) IMC-NST High High − − − J 39 1.9 cm (MRI) IMC-NST High Intermediate − − − K 33 4.3 cm (MRI) IMC-NST High High + + — L 44 8 cm (PE) IMC-NST High n/a − − − M 57 3 cm (US) IMC-NST High High − − − N 43 1.8 cm (US) IMC-NST High High − − − O 42 1.8 cm (US) IMC-NST High High − − − P 48 NDM IMC-NST High n/a − − + Q 45 3 cm (US) IMC-NST High High − + − R 50 2 cm (MRI) IMC-NST Intermediate Intermediate − − − S 55 3 cm (US) IMC-NST Intermediate Intermediate + + − T 43 2.9 cm (MRI) IMC-NST High High − − − U 36 1.6 cm IMC-NST Intermediate Low + + − V 65 4.6 cm IMC-NST Intermediate Intermediate − − + W 42 3.6 cm IMC-NST Intermediate Intermediate + + − X 56 n/a IMC-NST High High + + −
ER, estrogen receptor; HER2, human epidermal growth factor receptor type 2; ILC, invasive lobular carcinoma; IMC-NST, invasive mammary carcinoma, no special type; MRI, magnetic resonance imaging; NDM, no discrete mass; n/a, not available; PE, physical examination; PR, progesterone receptor; US, ultrasound.
Get Radiology Tree app to read full this article<
Acquisition Times
Get Radiology Tree app to read full this article<
Table 2
Scan Acquisition Times
Patient Start Times (Minutes After Fluorodeoxyglucose Injection) Prone-Supine Delay (min) Prone Supine A 64.48 77.25 12.77 B 61.05 72.78 11.73 C 64.8 76.28 11.48 D 70.38 85.73 15.35 E 58.05 79.23 21.18 F 61.15 73.17 12.02 G 71.02 81.23 10.21 H 60.23 71.75 11.52 I 61.88 71.62 9.74 J 64.27 75.32 11.05 K 62.48 73.00 10.52 L 64.5 74.95 10.45 M 62.48 73.00 10.52 N 54.5 65.98 11.48 O 55.32 65.82 10.50 P 59.98 69.83 9.85 Q 60.05 71.52 11.47 R 62.42 73.37 10.95 S 60.00 69.68 9.68 T 60.05 71.45 11.40 U 60.00 70.20 10.20 V 62.48 76.43 13.95 W 78.20 92.35 14.15 X 68.70 79.35 10.65
Get Radiology Tree app to read full this article<
Scan Quality
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Categorization of Anatomic Disease Distribution
Get Radiology Tree app to read full this article<
Table 3
Comparison of Prone and Supine Scanning for Categorization of Anatomic Disease Distribution
Patient Prone Supine Result Comments A Breast + axilla Breast + axilla Concordant B Breast + axilla Breast + axilla Concordant C BO-multifocal BO-unifocal Discordant Low-grade invasive lobular carcinoma, very low metabolic activity D Breast + axilla Breast + axilla Concordant E Breast + axilla Breast + axilla Concordant F Breast + axilla Breast + axilla Concordant G Breast + axilla Breast + axilla Concordant H Breast + axilla Breast + axilla Concordant I — — — Excluded because of part of axilla omitted from the field of view on prone scan J BO-unifocal BO-unifocal Concordant K Breast + axilla Breast + axilla Concordant L Breast + axilla Breast + axilla Concordant M Breast + axilla Breast + axilla Concordant N Breast + axilla Breast + axilla Concordant O BO-unifocal BO-unifocal Concordant P — — — Excluded because of part of axilla omitted from the field of view on prone scan Q BO-unifocal BO-unifocal Concordant R BO-unifocal BO-unifocal Concordant S BO-unifocal (bilateral) BO-unifocal (bilateral) Concordant T Breast + axilla Breast + axilla Concordant U Breast + axilla Breast + axilla Concordant V Breast + axilla Breast + axilla Concordant W Breast + axilla Breast + axilla Concordant X Breast + axilla Breast + axilla Concordant
BO, breast only.
Get Radiology Tree app to read full this article<
Assessment of Number of Involved Lymph Nodes
Get Radiology Tree app to read full this article<
Table 4
Comparison of Prone and Supine Scanning for Quantification of Involved Lymph Nodes
Patient Prone Supine Result Comments A 3 3 Concordant B 6 5 Discordant Better anatomic separation of deep structures on prone scan C — — D 1 1 Concordant E 7 4 Discordant Better anatomic separation of deep structures on prone scan F 4 3 Discordant Better anatomic separation of deep structures on prone scan G 2 2 Concordant H 1 1 Concordant I 7 8 — Excluded because of part of axilla omitted from the field of view on prone scan J — — K 2 2 Concordant L 2 2 Concordant M 2 2 Concordant N 1 1 Concordant O — — P 0 3 — Excluded because of part of axilla omitted from the field of view on prone scan Q — — R — — S — — T 1 1 Concordant U 9 5 Discordant Better anatomic separation of deep structures on prone scan V 3 3 Concordant W 4 4 Concordant X 2 2 Concordant
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Groheux D., Espie M., Giacchetti S., et. al.: Performance of FDG PET/CT in the clinical management of breast cancer. Radiology 2013; 266: pp. 388-405.
2. Hegarty C., Collins C.D.: PET/CT and breast cancer. Cancer Imag 2010; 10: pp. S59-S62.
3. Fletcher J.W., Djulbegovic B., Soares H.P., et. al.: Recommendations on the use of 18F-FDG PET in oncology. J Nucl Med 2008; 49: pp. 480-508.
4. Yutani K., Tatsumi M., Uehara T., et. al.: Effect of patients’ being prone during FDG PET for the diagnosis of breast cancer. AJR Am J Roentgenol 1999; 173: pp. 1337-1339.
5. Khalkhali I., Mena I., Diggles L.: Review of imaging techniques for the diagnosis of breast cancer: a new role of prone scintimammography using technetium-99m sestamibi. Eur J Nucl Med 1994; 21: pp. 357-362.
6. Moy L., Noz M.E., Maguire G.Q., et. al.: Prone mammoPET acquisition improves the ability to fuse MRI and PET breast scans. Clin Nucl Med 2007; 32: pp. 194-198.
7. Moy L., Ponzo F., Noz M.E., et. al.: Improving specificity of breast MRI using prone PET and fused MRI and PET 3D volume datasets. J Nucl Med 2007; 48: pp. 528-537.
8. Yankeelov T.E., Peterson T.E., Abramson R.G., et. al.: Simultaneous PET-MRI in oncology: a solution looking for a problem?. Magn Reson Imaging 2012; 30: pp. 1342-1356.
9. Li X., Abramson R.G., Arlinghaus L.R., et. al.: An algorithm for longitudinal registration of PET/CT images acquired during neoadjuvant chemotherapy in breast cancer: preliminary results. EJNMMI Res 2012; 2: pp. 62.
10. Wahl R.L., Siegel B.A., Coleman R.E., et. al.: Prospective multicenter study of axillary nodal staging by positron emission tomography in breast cancer: a report of the staging breast cancer with PET Study Group. J Clin Oncol 2004; 22: pp. 277-285.
11. Groves A.M., Shastry M., Ben-Haim S., et. al.: Defining the role of PET-CT in staging early breast cancer. Oncologist 2012; 17: pp. 613-619.
12. Heusner T.A., Kuemmel S., Umutlu L., et. al.: Breast cancer staging in a single session: whole-body PET/CT mammography. J Nucl Med 2008; 49: pp. 1215-1222.
13. Ravdin P.M., Siminoff L.A., Davis G.J., et. al.: Computer program to assist in making decisions about adjuvant therapy for women with early breast cancer. J Clin Oncol 2001; 19: pp. 980-991.
14. Recht A., Edge S.B., Solin L.J., et. al.: Postmastectomy radiotherapy: clinical practice guidelines of the American Society of Clinical Oncology. J Clin Oncol 2001; 19: pp. 1539-1569.
15. Aebi S., Davidson T., Gruber G., et. al.: Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2011; 22: pp. vi12-vi24.
16. Huang E.H., Tucker S.L., Strom E.A., et. al.: Postmastectomy radiation improves local-regional control and survival for selected patients with locally advanced breast cancer treated with neoadjuvant chemotherapy and mastectomy. J Clin Oncol 2004; 22: pp. 4691-4699.
17. Imbriaco M., Caprio M.G., Limite G., et. al.: Dual-time-point 18F-FDG PET/CT versus dynamic breast MRI of suspicious breast lesions. AJR Am J Roentgenol 2008; 191: pp. 1323-1330.